
1
2
3
4
5
6

7
8
9
10
11
12
13
14
15
16

Click to read if it interests you.
As if I needed another reason not to go to Portland
Who is accountable for Biden’s Autopen pardons? (and why it killed Iryna in Charlotte)
Obese surpass undernourished youths for first time, UN warns
Trump Mandates Transparency in Drug Advertising
‘Republicans Pounce’: Iryna Zarutska’s Murder Exposed the Left’s Inherent Contempt
Charlotte Pocketed $3.3M From Left-Wing NGO To Empty Jails For ‘Racial Equity’
Americans’ Wages Haven’t Kept Up With Inflation Since Biden Was Elected
A Texas doctor who defrauded federal health programs of $28 million as part of a massive $118 million scheme has been sentenced to 10 years in federal prison, the Department of Justice announced.
Dr. Jorge Zamora-Quezada, a rheumatologist based in Mission, Texas, falsely diagnosed hundreds of healthy patients with rheumatoid arthritis and subjected them to costly, unnecessary — and sometimes dangerous — treatments. His scheme targeted Medicare, Medicaid, TRICARE, and Blue Cross Blue Shield, stealing millions in taxpayer dollars meant to support vulnerable Americans.
Prosecutors said Zamora-Quezada operated a years-long fraud out of his clinic, using his medical license and staff — many of whom were foreign workers dependent on their employment visas — to fuel a lifestyle of luxury. He purchased a Maserati GranTurismo, a private jet, and 13 properties across the U.S. and Mexico, all while exposing innocent patients to toxic medications with serious, sometimes permanent side effects.
“Dr. Zamora-Quezada funded his luxurious lifestyle for two decades by traumatizing his patients, abusing his employees, lying to insurers, and stealing taxpayer money,” DOJ Criminal Division head Matthew R. Galeotti said.
So here’s the deal – remember when “experts” kept telling us what to do during COVID?
Turns out they got pretty much everything wrong. Like, spectacularly wrong.
We’re talking 19 major things they completely screwed up, from how the virus spreads to whether masks actually work (spoiler alert: those cloth masks were basically fashion accessories).
Dr. Fauci is the patron saint of TERRIBLE COVID policies.
He was wrong on SO MANY POINTS. It’s time to set the record straight…
Did he get anything right?
Last year the Norfolk Group just dropped a bomb of a document laying out all these failures. And it’s not just Monday morning quarterbacking – they’ve got the receipts. Real studies showing how natural immunity was actually legit (while Fauci pretended it didn’t exist), data proving schools could’ve stayed open (looking at you, Sweden), and evidence that maybe, just maybe, locking healthy people in their homes wasn’t the brilliant strategy they claimed.
Listen, I’m not here to say “I told you so” (okay, maybe a little), but we need to talk about this. Because if we don’t learn from how badly our “experts” messed up, we’re just asking for a repeat performance next time around. And honestly? I don’t think any of us can handle another round of plexiglass theater and double masking.
Let’s break down exactly how they got it wrong, and more importantly, why they kept doubling down even when the evidence said otherwise. Buckle up – this is gonna be a wild ride through the greatest public health face-plant in modern history.
These are the questions WE want answered!

Published2 hours ago
onApril 8, 2024
“It’s for humans too, you f*cking idiot.”
This is in response to the FDA’s infamous tweet: “You are not a horse. You are not a cow. Serious y’all. Stop It.”

Other facts the FDA ignored:


I mean, the headline says it all really. First, take it because it is safe and effective. Then, it was a pandemic of the unvaxxed. Stop blaming those of us educated enough not to get jabbed for your problems. I knew they were lying from the beginning about the mRNA lie.
I didn’t make anyone get jabbed. My position is everyone has to decide for themselves. The facts are coming out now, along with the consequences, but they were there the whole time.
A study published in August in the Journal of BioMedicine actually claims in its abstract:
Fear mongering and misinformation being peddled by people with no scientific training to terrorise people into staying unvaccinated is not just causing people to remain susceptible to viral outbreaks, but could also be causing more side effects seen in the vaccination process. This brief review will offer data that may demonstrate that misinformation perpetuated by the anti-vaccination movement may be causing more deaths and side effects from any vaccine.
Yes, apparently all those people suddenly dropping dead of heart attacks and strokes are being stressed into it by us anti-vaxxers warning them about heart attacks and strokes.
Now, if you’re thinking that’s the most ridiculous thing you’ve ever heard…well, you’re wrong. He’s done the research:
A mini review of published literature has been conducted and found that mental stress clearly causes vasoconstriction and arterial constriction of the blood vessels. Therefore, if subjects are panicked, concerned, stressed or scared of the vaccination, their arteries will constrict and become smaller in and around the time of receiving the vaccine.
See, they’re not dying because the vaccine gave them a heart attack…they’re dying because they were afraid it might.
Read the rest here, that’s all I could take, courtesy of Vlad Tepes, a blog you should follow
First, it would have saved a year and hundreds of thousands of lives. It would have eliminated the need for the mRNA jab.
What frosts my ass is that doctors went along with it because their licenses were threatened. They knew it would pass and a little rebellion would have held up the Hippocratic Oath.

And therein lies the problem. If you have a cure, you don’t need and Emergency Authorization for a jab that didn’t prevent catching or transmitting Covid to others. (Oh, and Ivermectin did too).
There are a lot of people that should be tried for murder or the prevention of healing through medicine.
This explanation is a little tough without a chemistry degree, but the average civilian can get the drift that it worked and would have saved more lives. I wouldn’t have killed those dying of Myocarditis and the upcoming diseases like SADS.
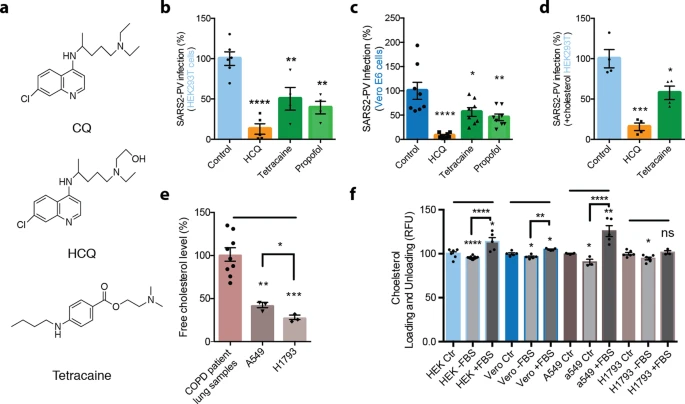
In order to test a membrane-disruptive mechanism for HCQ inhibition of SARS-CoV-2 viral entry, we compared HCQ to anesthetics (tetracaine and propofol) which are known to be membrane-disruptive. HEK293T cells overexpressing ACE2 were infected with a retrovirus pseudotyped with the SARS-CoV-2 spike protein (SARS2-PV). A segment of the spike protein binds to ACE2 and recapitulates viral entry47,48. A luciferase encoded in the pseudotyped virus is then used to quantitate viral entry (Fig. 1b–d).
Treatments with HCQ, tetracaine, and propofol all robustly reduced SARS2-PV entry into HEK293T cells overexpressing ACE2 (Fig. 1b). The cells were first treated with drugs (50 µM) for 1 h, then the drugs were removed. After the treatment and subsequent drug removal, SARS2-PV was applied such that the virus was never exposed to the drugs, thus avoiding potential direct effects of cholesterol on the viron. HCQ had the greatest effect on viral inhibition with almost a 90% reduction in SARS2-PV luciferase activity (Fig. 1b).
The study is linked above, but given that they all lied (see a post or two below) and the pattern appears.
A total of 72 observational studies, covering 1,976,099 patients, met the criteria for inclusion. Compared to those with sufficient vitamin D, the odds of developing COVID-19 among those with deficient or insufficient vitamin D levels were 1.46 times higher.
Their risk of severe disease was also 1.9 times higher, and their risk of death 2.07 times higher. One potential drawback was that all studies ranked “high” for risk of bias. The studies also differed in their definitions of severe illness and vitamin D deficiency/insufficiency, making absolute comparisons difficult.
Read the whole thing here. I didn’t do the study, but I know I’ve seen enough corroborating evidence that I’ve been taking it since I first heard of Covid.
One last nugget to send you over for the rest….
In the first of these four meta-analyses, “Prognostic and Therapeutic Role of Vitamin D in COVID-19: Systematic Review and Meta-Analysis,”3 published December 11, 2021, the researchers sought to determine “the association between vitamin D deficiency/insufficiency and susceptibility to COVID-19, its severity, mortality and role of vitamin D in its treatment.”
A total of 72 observational studies, covering 1,976,099 patients, met the criteria for inclusion. Compared to those with sufficient vitamin D, the odds of developing COVID-19 among those with deficient or insufficient vitamin D levels were 1.46 times higher.
Their risk of severe disease was also 1.9 times higher, and their risk of death 2.07 times higher. One potential drawback was that all studies ranked “high” for risk of bias. The studies also differed in their definitions of severe illness and vitamin D deficiency/insufficiency, making absolute comparisons difficult. That said, the authors concluded.
Why did the doctors recommend the jab instead of a cure? Of course I know to save their jobs because it sure as shooting wasn’t about science.
Of course it is. It always was. It doesn’t make vaxx money though, nor does it allow governments to pass crappy laws and control the population with fear and scare tactics. It is good to know that you can prevent it or be cured if you catch it.
Well, here it is. Decide for yourselves if you want myocarditis or thrombosis from the jab, or protection from Covid. You can order it from Amazon last time I checked.
Don’t believe the MSM, the government, Fauci, Gates, NIH, WHO, CDC, Fake book, Social Media, Google, Big Pharma or anyone else who stands to make money off of this.
Story begins here:
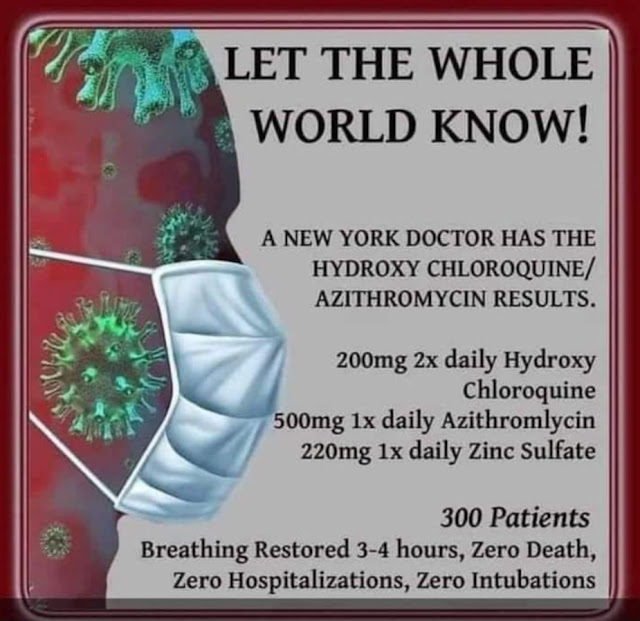
When it comes to the treatment of COVID-19, many Western nations have been hobbled by the politicization of medicine. Throughout 2020, media and many public health experts warned against the use of hydroxychloroquine (HCQ), despite the fact that many practicing doctors were praising its ability to save patients. Most have been silenced through online censorship. Some even lost their jobs for the “sin” of publicly sharing their successes with the drug.
Another decades-old antiparasitic drug that may be even more useful than HCQ is ivermectin. Like HCQ, ivermectin is on the World Health Organization’s list of essential drugs, but its benefits are also being ignored by public health officials and buried by mainstream media.
Ivermectin is a heartworm medication that has been shown to inhibit SARS-CoV-2 replication in vitro. In the U.S., the Frontline COVID-19 Critical Care Alliance (FLCCC) has been calling for widespread adoption of Ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19.
In the video above, Dr. John Campbell interviews Dr. Tess Lawrie about the drug and its use against COVID-19. Lawrie is a medical doctor and Ph.D. researcher who has done a lot of work in South Africa.
She’s also the director of Evidence-Based Medicine Consultancy Ltd., which is based in the U.K., and she helped organize the British Ivermectin Recommendation Development (BIRD) panel and the International Ivermectin for COVID Conference, held April 24, 2021.
What makes ivermectin particularly useful in COVID-19 is the fact that it works both in the initial viral phase of the illness, when antivirals are required, as well as the inflammatory stage, when the viral load drops off and anti-inflammatories become necessary.
According to Dr. Surya Kant, a medical doctor in India who has written a white paper on ivermectin, the drug reduces replication of the SARS-CoV-2 virus by several thousand times. Kant’s paper led several Indian provinces to start using ivermectin, both as a prophylactic and as treatment for COVID-19 in the summer of 2020.
In the video, Lawrie reviews the science behind her recommendation to use ivermectin. In summary:
As mentioned earlier, in the U.S., the FLCCC has also been calling for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19.
FLCCC president Dr. Pierre Kory, former professor of medicine at St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 2020, and the National Institutes of Health COVID-19 Treatment Guidelines Panel January 6, 2021. As noted by the FLCCC:
“The data shows the ability of the drug Ivermectin to prevent COVID-19, to keep those with early symptoms from progressing to the hyper-inflammatory phase of the disease, and even to help critically ill patients recover.
Dr. Kory testified that Ivermectin is effectively a ‘miracle drug’ against COVID-19 and called upon the government’s medical authorities … to urgently review the latest data and then issue guidelines for physicians, nurse-practitioners, and physician assistants to prescribe Ivermectin for COVID-19 …
… numerous clinical studies — including peer-reviewed randomized controlled trials — showed large magnitude benefits of Ivermectin in prophylaxis, early treatment and also in late-stage disease. Taken together … dozens of clinical trials that have now emerged from around the world are substantial enough to reliably assess clinical efficacy.
… data from 18 randomized controlled trials that included over 2,100 patients … demonstrated that Ivermectin produces faster viral clearance, faster time to hospital discharge, faster time to clinical recovery, and a 75% reduction in mortality rates.”
A one-page summary of the clinical trial evidence for Ivermectin can be downloaded from the FLCCC website. A more comprehensive, 31-page review of trials data has been published in the journal Frontiers of Pharmacology.
A listing of all the Ivermectin trials done to date, with links to the published studies, can be found on c19Ivermectin.com.
The FLCCC’s COVID-19 protocol was initially dubbed MATH+ (an acronym based on the key components of the treatment), but after several tweaks and updates, the prophylaxis and early outpatient treatment protocol is now known as I-MASK+ while the hospital treatment has been renamed I-MATH+, due to the addition of ivermectin.
The two protocols are available for download on the FLCCC Alliance website in multiple languages. The clinical and scientific rationale for the I-MATH+ hospital protocol has also been peer-reviewed and was published in the Journal of Intensive Care Medicine in mid-December 2020.
April 24 through 25, 2021, Lawrie hosted the first International Ivermectin for COVID Conference online. Twelve medical experts from around the world shared their knowledge during this conference, reviewing mechanism of action, protocols for prevention and treatment, including so-called long-hauler syndrome, research findings and real world data.
All of the lectures, which were recorded via Zoom, can be viewed on Bird-Group.org. In her closing address, Lawrie stated:
“The story of Ivermectin has highlighted that we are at a remarkable juncture in medical history. The tools that we use to heal and our connection with our patients are being systematically undermined by relentless disinformation.
The story of Ivermectin shows that we as a public have misplaced our trust in the authorities and have underestimated the extent to which money and power corrupts.
Had Ivermectin being employed in 2020 when medical colleagues around the world first alerted the authorities to its efficacy, millions of lives could have been saved, and the pandemic with all its associated suffering and loss brought to a rapid and timely end.
With politicians and other nonmedical individuals dictating to us what we are allowed to prescribe to the ill, we as doctors, have been put in a position such that our ability to uphold the Hippocratic oath is under attack.”
During the conference, Lawrie proposed that doctors around the world join together to form a new people-centered World Health Organization. “Never before has our role as doctors been so important because never before have we become complicit in causing so much harm,” she said.
Antiviral Research June 2020; 178: 104787
Evidence-Based Medicine Consultancy Ltd
Indian Journal of Tuberculosis July 2020; 67(3): 448-451
Antiviral Research June 2020; 178: 104787
Financial Express April 14, 2021
FLCCC January 7, 2021 Press Release (PDF)
FLCCC January 7, 2021 Press Release (PDF)
FLCCC Summary of Clinical Trials Evidence for Ivermectin in COVID-19 (PDF)
Frontiers of Pharmacology 2020 DOI: 10.3389/fphar.2021.643369
FLCCC Alliance I-MASK+ Protocol
FLCCC Alliance I-MASK+ Protocol
Journal of Intensive Care Medicine December 15, 2020 DOI: 10.1177/0885066620973585
Ivermectin for COVID Conference Speakers List
Bird-group.org Conference videos
Source: Epoch Times and the above links.


I see patterns, even someone from the Ivy Leagues could see this one also.
Many Western countries decided that the world must be Vaxxed, ignoring the obvious that HCQ and Ivermectin stop and cure Covid. To do so, they made both a villain. They all but outlawed them for use against the CCP virus and told doctors that they would lose their licenses if they prescribed a medicine that would heal sick people.
Let’s not ignore the fact that around 200 members of Congress used Ivermectin to cure themselves, the epitome of hypocrisy.

Thank God for Joe Rogan who exposed the hypocrisy and the lies told by government and the MSM. He took the “horse de-wormer” and surprise, he beat Covid in 3 days.
It’s come to light that aspirin can assist in the cure of the CCP/Wuhan Kung Flu virus:
A paper in Anesthesia and Analgesia published last spring titled, “Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019.”
This was a retrospective, observational study of adult patients admitted to multiple hospitals in the U.S. between March and July 2020, in the early days of COVID. The primary outcome addressed by the researchers from George Washington University was the need for mechanical ventilation, which then, and still now, carries an extremely high chance of never leaving the ICU alive.
This was not a gold standard randomized prospective clinical trial. That would not be feasible in this situation since study patients were already hospitalized and critically ill. Remember in the early days, one needed to be extremely ill before even being admitted to the hospital rather than being sent home until sick enough to return and go straight to the ICU.
The team investigated more than 400 COVID patients from hospitals across the United States who take aspirin unrelated to their COVID disease, and found that the treatment reduced the risk of several parameters by almost half: reaching mechanical ventilation by 44%, ICU admissions by 43%, and overall in-hospital mortality by 47%.
Although most patients with coronavirus disease 2019 (COVID-19) present with a mild upper respiratory tract infection and then recover, some infected patients develop pneumonia, acute respiratory distress syndrome, multi-organ failure, and death. Clues to the pathogenesis of severe COVID-19 may lie in the systemic inflammation and thrombosis observed in infected patients. We propose that severe COVID-19 is a microvascular disease in which coronavirus infection activates endothelial cells, triggering exocytosis, a rapid vascular response that drives microvascular inflammation and thrombosis.
HELP CURING THE VAX?
Aspirin Lowers Risk Of COVID: New Findings Support Preliminary Israeli Trial
The team investigated more than 400 COVID patients from hospitals across the United States who take aspirin unrelated to their COVID disease, and found that the treatment reduced the risk of several parameters by almost half: reaching mechanical ventilation by 44%, ICU admissions by 43%, and overall in-hospital mortality by 47%.
https://teamtuckercarlson.com/news/aspirin-lowers-risk-of-covid-new-findings-support-preliminary-israeli-trial/
Since aspirin helps those who have had strokes and heart attacks, it stands to reason that it would also help those who have contracted myocardial conditions and thrombosis caused by the jab.
But no, we can’t have that. It is against the diktat that everyone has to have the vax to be able to be able to function in society for everyday things like going to the store or flying. It doesn’t fit the narrative though.
ASPIRIN MUST BE BANNED IF IT WORKS
How did aspirin get its start? Over 3,500 years ago, willow bark, known as “nature’s aspirin,” was used as a painkiller and anti-pyretic by ancient Egyptians and Greeks, and in a chemical synthesis by a Bayer chemist in 1897.
HOW INTERESTING THAT NOW YOU SHOULDN’T TAKE IT FOR HEART ATTACKS OR STROKES
OTOH: Baby aspirin no longer recommended to prevent first heart attack in older adults, US task force says
People over the age of 60 should no longer consider taking a daily low-dose or baby aspirin to prevent a first heart attack or stroke, according to a draft recommendation issued by the U.S. Preventive Services Task Force Tuesday.
The announcement marks a change in the 2016 Task Force guidance that recommended aspirin therapy in certain men and women to lower cardiovascular risk. But more recent evidence suggests it also could cause harm, including bleeding in the stomach, intestines, and brain – a risk that increases with age and can be life-threatening.
https://www.uspreventiveservicestaskforce.org/uspstf/sites/default/files/file/supporting_documents/aspirin-cvd-prevention-final-rec-bulletin.pdf
This group is obviously one of the groups more likely to have more severe Covid reactions, those with a co-morbidity and over 60.
So. Not long after it’s discovered that aspirin, one of the best-known and longest-around medications there is, can significantly help reduce infection rates, hospitalizations, deaths, etc., and now the “conventional wisdom” suddenly shifts to telling people to avoid it? How… conveeeeeeeeenient.
I guess they don’t make enough money off of cheap and effective over the counter cures, nor do they achieve control over the masses.
Here is Singapore, almost fully Vaxxed.
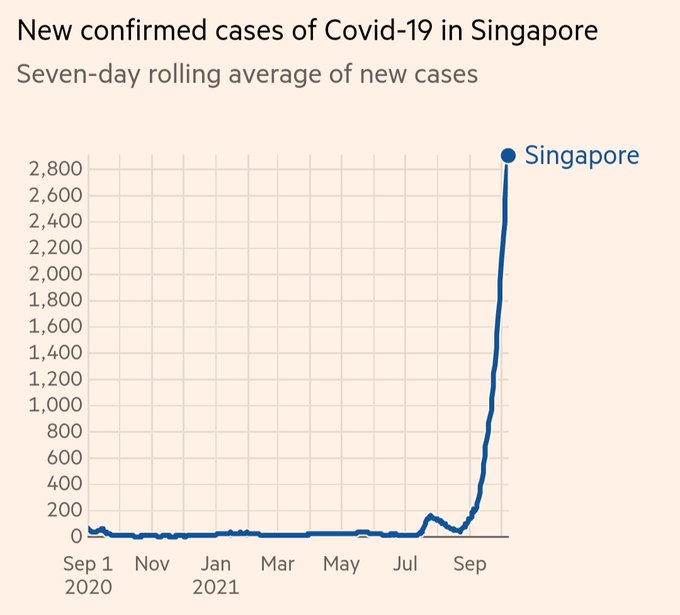
Here is Indonesia –
After the government authorized the use of Ivermectin for COVID-19 patients, the number of cases significantly plummeted since July.
The data below proves that Ivermectin played a role on the steep decline of COVID-19 cases despite having a low vaccination rate.
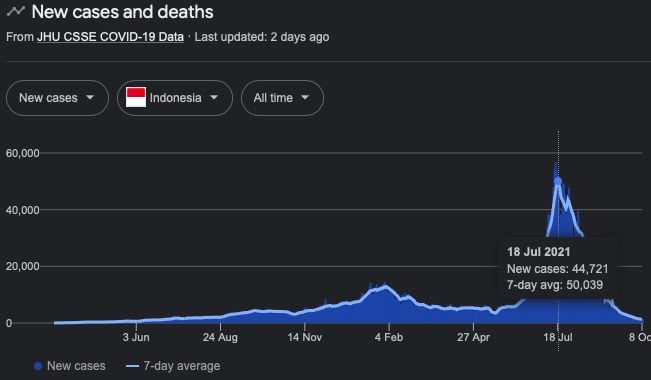
Here is a link to the data and story.
Do the math. Understand what works. Make an intelligent decision on your path. At least ask why they are forcing the Vax on us.
You do you.
What is the Hippocratic Oath?
Here is the first part:
| I swear to fulfill, to the best of my ability and judgment, this covenant: I will respect the hard-won scientific gains of those physicians in whose steps I walk, and gladly share such knowledge as is mine with those who are to follow. I will apply, for the benefit of the sick, all measures [that] are required, avoiding those twin traps of overtreatment and therapeutic nihilism. I will remember that there is art to medicine as well as science, and that warmth, sympathy, and understanding may outweigh the surgeon’s knife or the chemist’s drug. |
I guess it doesn’t apply if you don’t do what the Health SS says now.
DENVER (KDVR) — A patient on the kidney transplant list was moved to inactive status by UCHealth for not receiving a COVID-19 vaccine. Her living donor is also unvaccinated and UCHealth said both need to be vaccinated for the transplant process to continue.
The letter Leilani Lutali received states: “The transplant team at University of Colorado Hospital has determined that it is necessary to place you inactive on the waiting list. You will be inactivated on the list for non-compliance by not receiving the COVID vaccine. You will have 30 days to begin the vaccination series. If your decision is to refuse COVID vaccination you will be removed from the kidney transplant list. You will continue to accrue waiting time, but you will not receive a kidney offer while listed inactive. Once you complete the COVID vaccination series you will be reactivated on the kidney transplant list pending any other changes in your health condition.”
The Big Pharma are greedy for money from new medicines. Big Government is using Covid for the Re-Set with socialism and to take power and Bill Gates and the WHO want depopulation. Big Tech is covering simple and cheap solutions like this from everyone they can.
India said eff-you and gave everyone this and Ivermectin and have killed Covid off where it is used.
Wake up and stop the madness.



Here’s the article at the link but don’t bother. The real news is that Merck also invented and sells Ivermectin.
The story says it reduces hospitalization by 50%. That’s pretty good except that Ivermectin reduces it 100% if you look at the results of people taking it in India.
Why did they invent this pill? One, the vaxx isn’t working and kills people and two, Ivermectin is out of patent and there isn’t any money to be made.
It is experimental. The vaxx is still experimental and is still killing more people than Covid. I’m passing on this one.
Just give everyone the Ivermectin or HCQ and Covid is over. The problem for Big Pharma/Big Tech/Government is that their control and power grab would be over also.
By Nathan Jeffay 22 March 2021, 1:06 pm
Gilly Regev, an Israeli-raised scientist who co-founded the company SaNOtize, uses the new nasal spray she developed
A nasal spray that will be marketed as capable of killing 99.9 percent of virus particles has started rolling off production lines in an Israeli factory.
The spray could have prevented much of the world’s COVID-19 infection, its inventor, Dr. Gilly Regev, told The Times of Israel.
And more disturbing news is that I read there are HIV components in the mRNA vaccine.
Excerpt here:
So far, 18 sub-units of HIV1 have been found in the virus’ genetic code that cause the body to intentionally produce the HIV1 virus. “Could it give you HIV or AIDS? Nobody has the answer to that. Only time will tell; in years we will know. But you should know that there are people who tested positive for HIV after they got these vaccines… in Australia they tested positive. So this is something to be very concerned about.
There are cures out there now so why is there so much push for an unapproved jab? Your guess is as good as mine, but like Watergate, follow the money.
I went to a hospital today to have a procedure done. When the nurse apologized for the quantity of paperwork, I casually mentioned that things might become more complicated with Obamacare.
I was not ready for the answer. Actually, being in a very socially liberal city and healthcare system, I thought I was going to hear support for the program. I instead was told how government has corrupted the system, made it worse for both Doctors and patients and other horror stories. I replied that the government has not helped healthcare in a long time to which the nurse responded that the decline of morals in our culture was the beginning of the problem. How correct this nurse was.
Next, I met with the Doctor to go over what the procedure was going to entail. I again mentioned whether the healthcare system was affecting his job. Again I received a surprise answer.
The doctor told me of his passion for his practice all of his life. He then told me that what is being done to us by Washington has him considering getting out. He was honorable enough to not practice if he couldn’t do his best. It was a John Galt conversation. There are others like this doctor. I’ve found that if you are contemplating your retirement in your mind, you are already in the process of retiring.
To a person, the hospital staff admitted that Washington and the damage they have done and are doing to our healthcare system makes it worse for patients and providers. This is not a partisan statement for the record.
Let me point out that this was a highly successful practice with state of the art equipment and professional personnel making these perspicacious comments to me.
It was clear that they wanted to help people and do their job, but our own government is in the way. It seems obvious that they have overstepped their role in making sure that medicine is safe and lawful.
If I hadn’t heard it from the horse’s mouth, I wouldn’t have known. I did go in looking for a cure, but I left with a dose of information. It is easy to conclude that we need to fix or excise Washington from the healthcare system and put it back in the hands of the doctors.
After 18 years in private practice, many good, some not, I am making a very big change. I am leaving my practice.
No, this isn’t my ironic way of saying that I am going to change the way I see my practice; I am really quitting my job. The stresses and pressures of our current health care system become heavier, and heavier, making it increasingly difficult to practice medicine in a way that I feel my patients deserve. The rebellious innovator (who adopted EMR 16 years ago) in me looked for “outside the box” solutions to my problem, and found one that I think is worth the risk. I will be starting a solo practice that does not file insurance, instead taking a monthly “subscription” fee, which gives patients access to me.
I must confess that there are still a lot of details I need to work out, and plan on sharing the process of working these details with colleagues, consultants, and most importantly, my future patients.
Here are my main frustrations with the health care system that drove me to this big change:
Here are some things that are not reasons for my big change:
What will my practice look like? Here are the cornerstones on which I hope to build a new kind of practice.
This is the first of a whole bunch of posts on this subject. My hope is that the dialog started by my big change (and those of other doctors) will have bigger effects on the whole health care scene. Even if it doesn’t, however, I plan on having a practice where I can take better care of my patients while not getting burned out in the process.
Is this scary? Heck yeah, it’s terrifying in many ways. But the relief to be changing from being a nail, constantly pounded by an unreasonable system, to a hammer is enormous.
1- Find the C below.
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOCOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOOO
2- If you already found the C, now find the 6 below.
99999999999999999999999999999999999999999999999
99999999999999999999999999999999999999999999999
99999999999999999999999999999999999999999999999
69999999999999999999999999999999999999999999999
99999999999999999999999999999999999999999999999
99999999999999999999999999999999999999999999999
3 – Now find the N below. It’s a little more difficult.
MMMMMMMMMMMMMMMMMMMMMMMMMMMMNMM
MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMM
MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMM
MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMM
MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMM
This is NOT a joke. If you were able to pass these 3 tests, you can cancel your annual visit to your neurologist. Your brain is great and you’re far from having a close relationship with Alzheimer.


















{kind=link}