How short life is. It seems long, like in 3rd grade when I was waiting for school to end.
I’m at what will be my end in a few months. I’ve lived for decades and 2 different centuries, but like my Father told me on his 75th birthday, how did it go by so fast. I’ll never see that birthday number.
Since I’m saved, I’m not stressing over it, other than for my pets. I have family that will take care of my dog in case I go first. He’s starting to limp and might also be on his last couple of years.
I’d like to say something that would help others, but it’s going to be the same for everyone. You live, then you die, then you go to Heaven or Hell depending on your decision on forgiveness of sin.
As for me, anytime I feel something funny, like last night, I wonder how much time is left here. My time is all but over.
The cancer that is going to get me was completely a surprise, as was discovering it. That was an accident also.
Enjoy your family on this Holiday weekend. You never know when it’s your last. I do. I’m not going to see the next 4th of July, but at least I got to see the 250th Anniversary of our Country
The 4th of July for most on Earth is another day in the week, month year. Independence Day is when the greatest country was started.
For the readers of this blog, my medical diagnosis says that this will be my last one to celebrate.
I don’t want to get into it with internet pukes because what really matters is that it’s my Mom’s Birthday and the Day She died, July 4th. I’m also patriotic so I got lucky to grow up and live in the USA.
My mom was a patriot for God, but loved the USA. We were middle class and no more growing up. She lived through the depression so a dollar stretched to about $4.50 for our family. She had a masters degree in Education and Music, but chose to be a homemaker and a mother. That’s how I’ll remember her on this day.
Back to the original premise, we might have never made it to the moon, or invented air conditioning, cars, planes, trains and numerous medical advancements that have helped the world for the last 250 years.
I know haters shoot at #1, so it’s the Democrats who hate the good in our country. Hating America: The Hollywood Left’s Worst Anti-American Outbursts. You can see from the World Cup that the rest of the world woke up to the fact that the media lies about the good that the USA does for people primarily because of Trump (current excuse). The media are liars vying for power by means of thought and word, but they have been against anything that is right for the country and serve their leader, the devil.
Trump will go down as either good or bad, loved or hated or how ever he goes down in history, but he’s just a piece of the last 250 years of making the world better.
I stopped going to see my wife’s relatives in Europe because they just spout the media talking points about how bad we are. I was tired of their ignorance and prejudice as the Euro press possibly hates the US more than the Democrats. I don’t have to listen to it this way. I can read the European press and find out what her family would say to me. I have very little time left on Earth, I’m not going to waste it on people who are ignorant.
Europe is a museum now of what used to be great. The USA has been the leader in most things for decades. I bet the rest of the world gets tired of hearing the Star Spangled Banner every day at the Olympics or other global sporting events (I think soccer is a 2nd tier sport despite what the rest of the world tries to tell us).
So Happy Birthday Mom, and the rest of the world should be happy that we made it as a country, especially Europe around 1917 and 1940-45. It would be one big Germany otherwise. (She’s been gone 20 years now).
No country has invented more or helped more people medically, socially and historically. I’ll give you that the art from hundreds of years ago is better and looks good in the European museums, but they are static. People are working to invent new ways of doing things and curing illness (except Covid, that was a lie we told).
No other country has a hot dog eating contest on the 4th either.
Righteousness exalts a nation, but sin is a disgrace to any people. — Proverbs 14:34
Between 5 different doctors appointments, 2 procedures under anesthesia and so many blood draws that they used all my veins on both arms, I gathered these for those who care.
Profiles of Valor: Armed Forces Day – I always thank anyone in uniform or that has a hat from a previous war (especially Viet Nam) for their services. I include the Police, firemen, EMS, ICE, and anyone who thanklessly helps the public, especially liberals who hate them (and don’t know why, other than they were told to)
Honda reported its first annual loss since becoming a publicly listed company in 1957. The $2.7B drop comes months after the Japanese carmaker scaled back its electric vehicle plans in the US. (See the scrapped models.) – no free government handout, no one buys them. Gas price goes up, people buy Hemi’s
(Note: this is an update. Will B. Done pointed out that the links didn’t work, so I fixed them so you can click and enjoy)
I’ve written this blog since August of 2005. It was originally meant for my job in analyst relations, but took a turn when I retired in 2011. It’s morphed into any number of things from humor, sarcasm, anti-Covid Jab and my ramblings on life.
I start Chemotherapy next week, so it’s going to slow down considerably, although I’ll post from time to time. I’ve scheduled some posts so it will look like I’m continuing as I suffer through the poison they will be putting in me. You’ll read something every day this week, but I’m not collecting headlines. I hope to be back, I just know I won’t have any energy
I want to say that I’ve enjoyed the 10’s of thousands of comments, and different groups of readers.
I mostly wrote it as it is my favorite form of communication. If you read anything about me, you know I’m introverted so small talk isn’t my greatest strength.
I pulled the list of top posts. It’s funny to me that my most successful post is Euphemisms for Stupid, which was number one on Google for over 10 years in that category.
As I look at the list, I see various stages of my life and different careers. I see family, pets and co-workers. I’m especially proud of My Dad. It’s the post, On Behalf of the President of the United States.
I wish you all the best and a longer life than me.
It’s not over, but for sure will not be as consistent.
If anyone wants to guest post, send it to me simonize@protonmail.com and I’ll try to put it up and give you credit.
America’s reading habits by the numbers. (Explore) – It’s pitiful that that many people don’t read. No wonder many are falling behind. Books are some of my best friends
That’s easy. With my health problems, I’ll be a pile of ashes spread out somewhere.
Even though I’ll post it as a reminder, I’m going under the knife tomorrow morning. I’ve scheduled some stuff in advance, but I can’t promise much after Wednesday.
I may get headlines out tomorrow, but that will be the last day until probably the weekend.
Obama’s Tower of Doom Is Harder to Get Into Than America Itself – It doesn’t matter, no one is going to the South Side of Chicago anyway. No one gives a shit about Obama other than the media and the reverse racists, so it’s a waste of a billion dollars for the citizens of Illinois.
Maybe Star Trek fans can go look at it to see the closest thing to a real life Borg Cube looks like
So much for Allies
The Special Relationship Is Dead – France I get. They’ve fucked us as soon as Lafayette died. The UK used to have a backbone. Now, they have a Mosque. Time to pull out of NATO
Top 20 New Epstein Insights – Epstein isn’t an outlier but a byproduct of this system, connecting him to a continuum of state-sanctioned operatives we lovingly call The Blob. It’s more about intelligence than pedophilia.
Model City: Portland’s Journey From Symbol of Chic to Shabby – In 2012, it was keep Portland wierd. By 2018, it turned into a shithole with homeless and druggies everywhere. Now, people want to ge out and nobody wants to buy their houses or move there. It’s the liberal poster boy of how to ruin a good city
Mike Benz reveals the shadowy Obama bigwig who was secretly attached to Epstein…Name of the operator On the Obama team that went between countries and players. This is the secret spy stuff that goes on that they don’t want regular people finding out about. It even calls Clinton just a puppet while he was banging girls on Pedo Island.
Democrats Using Shutdown Threat To Rewrite Immigration Enforcement – It’s their new voter base because the Karen part of the party has taken over. No one other than people getting free stuff would vote for what they stand for. It’s going to ruin the nation. The republicans are letting them get away with it instead of standing up for the right thing and stopping it. Washington is broken….badly. These liberal women have to be stopped.
The Evidence Is Clear: Masks Don’t Do Anything… – neither did the jab or social distancing. It was just controlling the population. The Germans did shit like that in the 30’s and everyone obeyed like sheep. They could have just taken vitamin D3 and ivermectin and be protected for a few cents.
Not that flying hasn’t been on a trend that sucks worse every time, now it’s coming out that the jab is harder on the hearts of pilots than others, and they are having problems. The last thing I need is a pilot who has died suddenly in the cockpit.
A couple of excerpts and then the whole story:
Well, what I learned is scientifically proven that pilots are suffering myocarditis and pericarditis at rates higher than what the CDC said the natural average should be for those who took the vaccine, and considerably higher.
Walker worries that pilots are already at increased risk for blood clots at flight altitudes— and that’s also one of the risks of Covid vaccines. She’s trying to get her study under the nose of important members of Congress and the FAA to address.
Story:
As air travel soars, lingering fears about Covid vaccine side effects cast a shadow over aviation safety. Passengers wonder if their vaccinated pilots could face sudden mid-air health crises. A 2022 survey revealed 23% U.S. commercial and military pilots reported adverse effects, including heart inflammation, which can trigger sudden death. Sherry Walker, a researcher and a captain at a major airline, warns that official responses have sidestepped concerns, leaving critical questions about pilot health unanswered.
The following is a transcript of a report from “Full Measure with Sharyl Attkisson.” Watch the video by clicking the link at the end of the page.
Sherry Walker: So it dawned on me that if we don’t get true scientific study, if we don’t get to the bottom of the issue, then that could harm my industry, which obviously I enjoy flying and I make a living at it. And if there is a problem, we’re allowing these people to suffer in silence.
She says she devised the Oklahoma State Pilot Study and brought it to a large industry meeting in 2021.
Walker: I walked around for four days with a QR code and a T-shirt that said “Oklahoma State Pilot Study” on it and begged and pleaded. And then I listened to the stories of the people who knew somebody. So we went from about a hundred surveys to 1,422 responses shortly thereafter.
Sharyl: What did you learn?
Walker: Well, what I learned is scientifically proven that pilots are suffering myocarditis and pericarditis at rates higher than what the CDC said the natural average should be for those who took the vaccine and considerably higher.
Sharyl: What kinds of stories or anecdotes did you hear?
Walker: Well, a lot of pilots or the latter category, “oh my gosh, I’m having issues with my heart.” One dear friend and I said, “you need to ground yourself. You need to go to the doctor now.” “Oh, I can’t because then I can’t feed my kids and this and that.” And so, so we learned a lot of that.
Sharyl: Did you get vaccinated?
Walker: No.
Sharyl: How did you manage to avoid it working as a commercial pilot?
Walker: It was a company mandate and my husband, myself, 2000 other employees of my company and put in religious and or medical accommodation requests, and then we were effectively terminated. And then we went to court and in February of 22, the fifth circuit reversed and we were called back to work. By then the contractor mandate and the OSHA mandates had fallen in the courts. So the pandemic was effectively over and we all went back to work.
Sharyl: In the big picture, what do you think this tells us?
Walker: So what I proposed in my study was, additional oversight, some congressional requirements to allow, mandate that the FAA take a look at this, ask the question of pilots, “are you vaccinated or unvaccinated?” Not because we wanna stop pilots from flying, but those frontline doctors that can treat or can recognize problems in advance can educate the pilot and say, “Hey, if you did and you see this, you might want to consider that.” So, but it’s all, you know, heads in the sand right now.
Sharyl (on-camera): Walker worries that pilots are already at increased risk for blood clots at flight altitudes— and that’s also one of the risks of Covid vaccines. She’s trying to get her study under the nose of important members of Congress and the FAA to address.
Of course I do. We were made to get nutrition from omnivorous sources. When younger, I harvested my own meat and vegetables, and took care of 60 animals for every one that fed my family.
Now, I eat only organic, unprocessed foods. After all, you are eating what your meal ate. It is for cardiovascular reasons.
Your body requires specific energy sources that vegetables alone cannot provide.
If I meet a vegan cat lady, I will know it’s a red flag for an unhealthy person, both in mind and body. Stay away from these people, very far away.
It’s better than eating the insects the WEF want us to eat, pricks.
This was written by Dr. Philip Ovadia. A link to contact him is provided below
Some doctors dub it “holiday heart.” Others refer to it as HHS. But no matter what you call it, the data is clear: more people die of heart attacks during the holidays than any other season.
Research in Sweden found a 15% increase in heart attacks for the winter holidays, with a spike of 37% on Christmas Eve. It’s especially high risk for people over 75, those with diabetes, or anyone who’s suffered from cardiovascular disease.
Please know that I’m not saying this to scare you. I just want you to enjoy the holidays without sabotaging your metabolic health.
Knowing your risks is half the battle.
So here’s what you should know, plus how to keep your heart in check.
Reducing your heart health risks during the holiday season
Does the holiday season inherently raise your risks for heart disease? No. But does it become more difficult to manage risk and avoid metabolically unhealthy practices? Most definitely.
Fortunately, there’s quite a bit you can still control.
Let’s take a look at some of the risk factors below.
Cut sugar
You don’t need to be a rocket scientist to realize sugar intake climbs during the holidays. Between the cakes, cookies, and pies, it’s hard to say no to the comforts of the season. It may be harder on those with existing metabolic conditions. One study following diabetics in the post-holiday season found that glycemia and lipids do increase after the festivities are over.
But as we know, sugar consumption does no favors for the heart. High consumption is directly linked with heart failure, diabetes, stroke risk, and even neurodegenerative diseases such as dementia.
I’m not saying you should cut all sugar during the holidays — just make better choices to protect your metabolic health. This might be swapping to whole, real alternatives such as honey instead of corn syrup. There are some sugar alternatives, but be advised fake sugars come with potential health risks.
I realize it can be hard to avoid sweets at gatherings with family and friends, especially if they’re not necessarily supportive of your efforts.
But I highly recommend doing your best and cutting sugar to whatever extent that means for you.
Monitor processed foods
The holidays (quite literally) bring all sorts of processed foods to the table. Prepackaged sweets, sausages, pies, and baking mixes promise to add “the flavor of the season” to your dining room table. And considering 73% of the US food supply is made up of processed foods, there’s a good chance UPFs will be present during at least one of your holiday events.
It is still possible to enjoy holiday classics with whole, real food once you master simple cooking skills.
Manage stress
I don’t need to remind you just how stressful the holidays can be. Two in five people say their stress increases during the holidays, with fears about money, travel, and busy schedules topping the list.
I realize there’s no way to eliminate stress during the holidays completely, but chronic levels can increase many heart health risk factors. They may also encourage poor habits, such as smoking, binge drinking, or poor sleep.
I highly encourage you to find time for yourself, set up relaxing routines, and seek support when needed. You can also get more specific advice around this in my guide covering how stress increases your risk for heart disease.
Keep yourself warm
Cold weather forces blood vessels to constrict, which can increase your blood pressure and put more strain on your heart. For those with a history of chest pain, this can lead to (or worsen) angina. In extreme circumstances, it could limit blood flow to the heart.
Keep in mind that cold weather may also affect the viscosity of your blood. It may be thicker and stickier, which makes it more likely to form clots. This ultimately raises your risk of heart attacks and strokes if you’re already at risk or have a history of heart problems.
Be conscious of your drinking
I’m not a fan of alcohol at the best of times — even one glass a day contributes to poor metabolic health. Apart from increased blood pressure, drinking can also spike your blood sugar and increase your risk of heart disease. Yes, this applies to holiday favorites like hard ciders and eggnog.
Drinking too much alcohol can also lead to arrhythmia, or an irregular heartbeat, that lasts for many hours. That’s actually where the term “holiday heart syndrome” came from in 1978.
So I recommend limiting alcohol significantly and looking for alternative celebratory drinks. But if you’re struggling to pull back, start with baby steps first. Maybe this means one fewer glass before going to bed, or experimenting with non-alcoholic versions of your favorite drinks.
Make activity a priority
Between the weather, holiday movies, and potential long-distance travel, people are typically far less active during the winter months. This can certainly raise your long-term heart health risks. But there are also some short-term risks to consider: namely, deep-vein thrombosis.
Thrombosis occurs when blood clots form in a vein or artery, usually within the leg. There are a multitude of factors that contribute to clot formation in the case, but one of the most common is immobility — being unable to move around for long periods of time.
You may be immobile while working a desk job, sitting in a car or plane, or sitting down on the couch to watch the Hallmark channel. These things aren’t inherently ‘bad’ per se, but in an already inactive season fraught with cold weather, your risk factors will be higher.
Do your best to continue some semblance of an exercise routine, perhaps extra movement sprinkled in (like an after-dinner walk, for example). I understand it might feel awkward or embarrassing to continue a routine around friends or family, so you may want to check out these four ways to strengthen your heart when you don’t have time to exercise.
A final note
This isn’t, I’m sure, the most exciting thing to read before the holidays. And yet, as a heart surgeon, I care too much not to say something.
Please understand I’m not asking you to moderate your fun, or give up things you enjoy during this special time of year. The purpose of my content is to give you information, so you can come to your own conclusions and make decisions to improve your quality of life.
If you’re interested in learning more about the intricacies of your heart health, I highly recommend the following resources:
BREAKING STUDY: Anomalous Amyloid Microclots Found in 100% of the COVID-19 Vaccinated – So it was never safe and effective, they lied. Those 20% of us who didn’t get jabbed never have to regret this. It’s funny that people told me who felt sorry for me when I said I didn’t get vaccinated. How the tables have been turned. We’re not even into the long-term effects yet
The 10 Coolest Cars at the 2025 Los Angeles Auto Show – Not exactly my idea of cool, but it sure is for somebody. I might have thrown in a Bugatti Chiron, A W-18 Porsche, but the first couple are cool. The Fiat is lame
I somehow was blessed with an innate ability for pattern recognition. I can see disparate things happening, put them together, and know what a good opportunity is. I didn’t know it until things fell into place for me, and I thought everyone saw what I did, but I was wrong.
Here are a couple of examples. I’ll be as matter-of-fact as I can.
I chose a career in personal computers when I didn’t know what to do. They couldn’t do anything, except for VisiCalc, but I saw it as my future before they introduced the IBM PC. The head of a major company said he saw a demand for about 5 of them, and why would you want one on your desk. I made a career out of it. People thought I was chasing my tail at the time.
I had things in life I wanted to do, and knew that if I wanted to retire by 55, I’d have to start before 30. I finally left at 53, and people at IBM were still living paycheck to paycheck up in NY. I refused two job offers to move there to live where the cost of living was 30% less. Money is made 2 ways: make more and spend less. I did both. Plus, I didn’t have to live in NY.
It was clear to me that COVID was a hoax from the beginning, and I refused the jab when the sheep were lining up for it. Once I saw that the Government was forcing an untried and untested treatment they called a vaccine, I knew not to take it. I had studied gene editing and knew it was untested and untrustworthy. My whole family and all my friends thought I was nuts. They couldn’t wait to get it and thought I was risking my life by not getting it. They all got Covid anyway.
My Son in Law, who has patents and is a chip designer said I was smart, so why didn’t I get it? I’m not a lemming, that’s why. It was clear to me that Ivermectin and Hydroxychloroquine were the cure. They tried so hard to ban (and got the media to promote that it was bad) it that I knew to research it and found it to be the cure. I never regretted not getting jabbed, and the rest of the family now wishes they had made my decision. They rushed to get it because they were told that it was “safe and effective”. I called BS. We don’t talk about it because they hate me being right on that one. Thanksgiving is next week, and it will come up like Trump.
I never doubted that Trump would beat Hillary when Scott Adams talked about his ability to use persuasion techniques. I was an island on that one also. I was less certain in 2020, as the evidence of rigging and judicial interference was too overwhelming. Anybody could have called the 2024 election, so I don’t take any credit.
I worked in sustainability for IBM around 2009, but I knew Climate change was a scam when they worried about the hole in the Ozone layer in the late 1990’s. I knew it was a lie from the start, and we found out this week from none other than Bill Gates that it isn’t true, but rather a power grab. I read yesterday that the Ozone hole was mysteriously closing. Again, I was on an island calling BS.
I also have spatial Awareness that I got from my father. I can see how things fit together. It’s as clear as day when others are just arranging objects. Between that and pattern recognition, some things are clear to me as to their truth or the path I should take.
The Make America Health Again (MAHA) movement has made quite a few waves in 2025. And by the end of the year, it will make at least one more: HHS Secretary Robert F. Kennedy Jr. has announced new dietary guidelines that will revise or revamp existing Dietary Guidelines Advisory Committee (DGAC) reports.
While these new dietary guidelines have yet to be released, we have quite a few details on what to expect. Some people believe they may be misleading or even dangerous. But as a cardiologist and heart surgeon of 30+ years, I’m very optimistic they will help reduce our rates of heart disease.
Below, I break down the most important principles to know, plus the guidelines’ ramifications for American heart health.
One quick note: this is not intended to be political commentary. There are plenty of party-based perspectives on these dietary guidelines, and lots of opinions from all sides. My goal here is to examine the facts and provide my honest perspective.
RFK guidelines versus traditional nutrition advice
First, a little background.
The Dietary Guidelines Advisory Committee releases an updated nutrition guideline every five years. This is a 400+ page report you can access at dietaryguidelines.gov, although it isn’t intended for public use. Rather, it’s a boilerplate of Federal guidelines for things like school lunches, military rations, and government assistance programs.
But RFK’s guidelines are set to be significantly shorter — just four to six pages. The goal is to create a set of “common sense guidelines” that anyone can use to make decisions about their nutrition.
Again, the guidelines themselves have yet to be released. But we have a pretty good idea of what they’ll include.
Here’s a closer look at some anticipated changes so you can compare and contrast with traditional guidelines.
Emphasizes whole, real foods
Traditional dietary guidelines such as the food pyramid and MyPlate categorize foods by the nutrients they provide.
So for example:
6 servings of grains
2 servings of protein
2.5 servings of vegetables
3 servings oils and fats
What it doesn’t account for is the qualities of these foods, or how processed they are. Fruit and gel cups still count as a serving of “fruit,” while sweetened yogurt tubes and Goldfish count as dairy and grains, respectively.
You don’t need to be a nutritionist to realize this leaves a very large gap for interpretation.
Because people don’t eat nutrients, they eat food.
RFK’s proposed guidelines help eliminate this confusion by emphasizing whole, real foods over arbitrary classifications (like whether or not you got your “servings” of grain today). This is also much more scientifically sound; it goes beyond categorizing nutrient types and makes it easier to isolate ultra-processed foods, or UPFs.
The current administration plans to develop a “government-wide definition” for ultraprocessed food. This likely means a working definition for whole, real food as well.
In my opinion, establishing a definition for ultra-processed foods is a net positive for everyone. Not only will people know how to better avoid unhealthy options, but they can also significantly decrease their risk of heart disease.
Encourages more saturated fat
While RFK’s new dietary guidelines won’t focus much on specific nutrients, there is one component likely to be emphasized more than others. In his own words, “[these] new dietary guidelines that are common sense, that stress the need to eat saturated fats of dairy, of good meat, of fresh meat.”
RFK has gone on record multiple times explaining that animal-based products deserve a higher priority in the everyday diet. But animal-based products contain more saturated fat — something of a boogeyman in traditional guidelines.
If these new guidelines do raise suggested intakes for saturated fat, it will go against decades of advice from the US DGA, and this is concerning some nutritionists. For context, traditional US guidelines recommended an intake of 10% of daily calories. The American Heart Association recommends even less, around 6%.
But we don’t have any evidence to suggest that limiting saturated fat intake actually prevents heart disease. Plus, increasing saturated fat intakes from whole, real sources is unlikely to negatively affect heart health. If anything, it may improve it.
That’s because some of the highest sources of saturated fat in the US are pizza and ice cream. Sandwiches, desserts, and sweet snacks aren’t far behind. These are ultra-processed foods that will have other, more serious ramifications (like spiking your blood sugar, for example).
So what does this tell us? That whole, real foods like steak and eggs are not primary sources of saturated fat in the average American diet.
Demystifying saturated fat from whole, real food sources will play a substantial role in improving dietary quality and heart health.
What I’d like to see: A heart surgeon’s perspective on food guidelines
Contrary to popular belief, RFK Jr’s proposed dietary guidelines do not work adversarially to supporting heart health. I don’t say this flippantly, either: I am firmly dedicated to Making America Healthy Again, and will (and do) only support changes that match my research and opinions.
Here are the other components I would love to see added:
Firmer guidelines about alcohol consumption. Alcohol is not your friend, and it certainly doesn’t do any favors for your heart. Adding educational information about how drinking interacts with heart health could be extraordinarily beneficial to those wanting to reclaim their metabolic health.
A heavier emphasis on animal products. Many animal-based products make a world of difference in heart health maintenance and heart attack recovery. My hope is that the guidelines demystify animal products so they can become dietary staples instead of guilty pleasures. For example, eggs, milk, and ruminant meat such as beef, lamb, and venison.
Education about limiting carbohydrate intake. People deserve to know how carbohydrates affect their bodies, and how overconsumption can lead to insulin resistance, inflammation, and heart disease. While not everyone needs to follow a low-carb diet, adding some concise information about how to avoid unnecessary starches could be enormously effective in limiting overconsumption.
Time will tell what the guidelines contain. We don’t have long to wait: they’re slated for release no later than the end of this year.
As we wait for its release, I highly encourage you to perform research of your own. I’ve written quite a few guides covering nutrition and heart health you can use to get more information.
Researchers have done a significant amount of work exploring the gut-brain axis, or how the food we eat affects the way we think. But they’ve also spent time exploring the gut-heart axis — which, in my opinion, is one of the most important biological concepts of our generation.
The food you eat has a direct impact on the heart, both directly and indirectly through your gut microbiota.
I’m going to take the next few minutes to discuss how this interaction works, as well as what you can do to improve your gut (and heart) health over time.
Exploring the gut-heart connection
The state of your gut bacteria — as well as nutrients, compounds, and hormones it produces — has an impact on your heart.
First, the nutritional aspects.
We know the heart receives priority nutrients from our diets, especially from the fats we eat. Studies suggest that the heart directly receives nutrients through blood after digestion. This is because blood from the small intestines, where digestion takes place, collects in the hepatic portal vein. Blood passes directly from the intestines to the liver, then to the inferior vena cava and the heart. This means the heart receives some of the first and most intimate contact with nutritious (or not so nutritious) food you’re consuming.
We also know your gut bacteria produce more than just nutrients. As they break down certain foods, they also create secondary compounds called metabolites. These include:
GABA
Amino acids like tryptophan and tyramine
Trimethylamine N-oxide
Noradrenaline
Dopamine
Serotonin
Studies show that dysregulated metabolite production can “activate pathways that promote myocardial injury and may contribute to ventricular dysfunction” (in other words, encourage heart disease).
It can also lead to inflammation. This is the third and biggest way your gut contributes to heart disease.
Here’s a flyby overview of how this works:
Your intestinal lining is semipermeable to allow for adequate digestion.
But poor gut health, known as leaky gut, allows for hyperpermeability, or a large amount of exchange between your intestines and bloodstream. Leaky gut can also stem from conditions such as SIBO and PCOS.
Leaky gut stimulates inflammation in your body by quite literally leaking toxins into your bloodstream (including high-sugar food).
This puts your body into a state of systemic or chronic inflammation, meaning it doesn’t go away on its own.
This gut inflammation directly impacts the heart by causing blood vessels to become stiff, hard, and narrow. It may also accelerate plaque accumulation, which greatly contributes to heart disease.
So what does all this mean? That your next bite of food could have a major impact on your heart.
And if you’re not eating nutrient-dense, whole, real food, it will also be one of the first organs to bear the brunt of damage.
How to improve your gut-heart axis
There’s no overnight fix for your gut or your heart health.
But there are certainly steps you can take to see results faster.
This includes:
1. Whole, real food
The first piece of the puzzle is changing what you eat.
The amount of sleep you get each night can have a dramatic effect on your gut’s microbial health. The less sleep you get, the less diverse your bacteria are. Dysbiosis can also affect the quality of your sleep, which creates a vicious cycle. Namely, one that affects your heart.
Getting seven to nine hours per night is considered key to metabolic health. You might need more or less depending on age, health, and activity level, but it’s still a target to hit, alongside many of the other principles of metabolic health.
3. Reassessing medications
If you can’t eliminate medications, you may consider supplementation as a way to support your gut health.
The following is a list of bioactive compounds known to support the gut-heart axis:
Polyphenols: These are plant compounds found in substances like berries and tea.
Prebiotics: Onions, garlic, leeks, and asparagus are good examples.
Probiotics: Yogurt and kefir are some of the most common, although sauerkraut and kimchi are also options.
Quercetin: Red onions and capers contain quercetin, among many other plants.
Resveratrol: Blueberries are often the most common example.
Some dietary fibers: This includes vegetables like broccoli and leafy greens.
4. Cutting sugar
Sugar not only changes your gut microbiota, but also fundamentally damages your liver, pancreas, and blood sugar function.
Your best bet is eliminating processed sugar altogether, although I realize that can be a struggle depending on where you’re at.
First, reduce your consumption. Rather than three sodas a day, make it two. Then, look for sugar alternatives. Instead of processed sweets before bed, you might try fruit, milk, or berries. You can also try wearing a CGM to assess how your blood sugar responds to these alternatives in real time.
Finally, reduce the amount of processed carbohydrates you eat. Substances like bread and alcohol, for example, turn into sugar in the bloodstream.
Speaking of fat, we also know fat consumption contributes heavily to heart health. Research has found that “increasing fatty acid availability to the heart results in a marked inhibition of glucose oxidation,” leading to healthier function.
This is especially true of ketones, or a type of fatty acid that is beneficial to heart health. Ketones directly affect the mammalian target of rapamycin (mTOR) signaling, which is a bodily process affecting cardiac function, cellular growth, and insulin sensitivity.
They lied about Gain of Function. They lied about the vaccine being safe and effective for preventing Covid-19. They lied that it would prevent the spread. They lied that masks would work. They lied that you had to be jabbed to keep your job.
Now, the test results show that the PCR test to detect Covid-19 was just as big of a lie. The results were fake and mostly wrong.
We all remember mid-2020 through all of 2021 when every news channel, it seemed, had a running scoreboard with the daily infections and daily deaths allegedly caused by COVID-19, remaining pinned as a sidebar even when the stories being covered were wholly independent from the ‘pandemic’.
The entire COVID-19 hysteria was exacerbated by widespread testing at the urging of global non-profits and non-governmental organizations and at the U.S. taxpayers’ expense. So long as the Mockingbird Media could increment those “Daily Infected” numbers each night for primetime television.
Scientific organizations such as Science.org criticized the U.S. for inadequate testing in late February 2020, comparing the 1.6 million tests-per-week capability of China with just “459 tests since the epidemic began” in the United States.
That publication went as far as quoting an In-Q-Tel employee, Luciana Borio, saying that the “CDC normally ‘gets the ball rolling’ with diagnostics because it has the expertise and the biosafety laboratories to handle dangerous novel level pathogens. In-Q-Tel was the “first government-sponsored venture capital firm” chartered by the Central Intelligence Agency.
A PubMed editorial in December 2020 stated that, “The number of positive molecular diagnostic tests, which are largely based on real-time (RT) PCR assays that detect genetic material of the causative agent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), still forms the basis for reporting both symptomatic and asymptomatic cases worldwide.”
The Nobel Prize-winning biochemist who invented the polymerase chain reaction (PCR) in 1983 had previously warned several times that PCR “can find almost anything in anybody”. Of course these statements were quickly “fact-checked” and “debunked” by outlets like USAToday and The Journal, mainly claiming the cited quotes were “missing context” and that Mullis was specifically referring to the HIV virus and that “health experts say PCR tests are accurate and reliable in detecting COVID-19.”
But a new study out of Germany suggests the testing and dramatic sidebar counters were (mostly) wrong.
Last month, Frontiers in Epidemiology released a peer-reviewed study that obliterated the COVID-19 infection claims that were promulgated to the masses via mainstream news ‘sidebars’ and daily reports on new infections.
We analyzed the ALM-observed week-resolved time courses of test-positive fractions of PCR and IgG tests… Specifically, we show that scaling and shifting the cumulative sum of previous PCR-positive fractions effectively reproduces the time course of the IgG-positive fraction. The value of 0.14 found for the fitted scaling parameter means that only 14% of those who were tested PCR-positively actually became infected with SARS-CoV-2. This parameter fit further implies that a quarter of the German population already carried IgG antibodies from natural infections in their blood at the turn of the year from 2020 to 2021.
The Summary and Conclusion states that:
The principal finding from our analysis of ALM data on both nucleic acid amplification (PCR from mucosal swabs) and IgG antibody (serological) testing for SARS-CoV-2 in Germany between mid-March 2020 and summer 2021 is this: only 14%—and possibly even fewer, down to 10%—of individuals identified as SARS-CoV-2-positive via PCR testing were actually infected, as evidenced by detectable IgG antibodies.
…This evidence-based and representative serological signal was disregarded in favor of relying on the weekly absolute number of positive PCR tests—the so-called “7-day incidence” (“Sieben-Tage-Inzidenz”). Unequivocally, this definition of incidence yields a scientifically meaningless figure in the context of infection dynamics, as it depends entirely on the arbitrary (or imposed) number of PCR tests performed. It is therefore not an objective indicator of epidemiological reality, but an administratively imposed figure—more reflective of political will than scientific rigor. Yet, incomprehensibly, this 7-day incidence metric was even incorporated into the German Infection Protection Act (“Infektionsschutzgesetz”) as the quantitative foundation for imposing highly restrictive public health measures. The methodological shortcomings and institutional processes that enabled its elevation to policy status demand critical re-evaluation—not only to prevent similar errors in the future, but to restore trust in evidence-based public health governance.
This German study tears apart the force-fed narrative. The PCR numbers were as fake. They were used to scare people and justify draconian lockdowns that greatly increased the financial gaps in society, hammering down the middle and lower class while creating exorbitant wealth for the top corporate oligarchs.
P1 with Matt and Tommy, Late Breaking F1, Things Unseen – Sinclair Ferguson, Wisdom for the Heart – Stephen Davey, The Move – Lance Armstrong, Cycling podcast, Wicked Smart Golf, The Race F1 podcast, History extra, We we have ways of making you talk, James Allen, Bring back V10’s, Dr. Hyman podcast, Stay off my operating table – Philip Ovaida, Jefferson Fisher, The rest is his story, The Red Pilled America, Missed Apex F1, The Chequered flag, Parc Fermé, Sharyl Attkisson.
I started out watching 24Cast. I loved Jack Bauer saving the day. I was heavily into martial arts at the time, and Jack was ex-Delta Force. It quickly went to F1 and Christian sermons that were meaningful to me.
I used to listen to the Marvel and Star Wars podcasts, but those shows went woke, so I lost interest. Agents of S.H.I.E.L.D. ended so that took care of itself.
I miss F1 Misfits though. It was 2 Aussies with a sense of humor which used to kill me. They just went away. I listened to almost 1000 episodes of F1Weekly, but Clark lost the passion and just goes through the motions so I stopped.
I go in and out depending on what my interests are, but I can fall asleep to any of them.
Scientists at St. Jude Children’s Research Hospital explored how mutations in mitochondrial DNA contribute to cancer, the extent of their impact, and when and how they become a factor. Mitochondria act as energy factories in cells and have their own, separate DNA. Mutations to mitochondrial DNA (mtDNA) have been observed in cancer, but it has been unclear how these changes might affect cancer growth. To find answers, St. Jude Children’s Research Hospital scientists combined computational tools and DNA sequencing technologies to examine these mtDNA mutations in cancer cells closely. Their new method lets scientists pinpoint when these mutations occur, how they change as cancer develops and whether they affect how cancer cells behave. The results of this study were published today in Science Advances.
Exploring the role that individual mtDNA mutations have on cancer has historically been difficult. “Each cell contains hundreds of copies of mitochondrial DNA; so, a mutation might be present at low levels in many cells, or at high levels in just a subset of cells,” said corresponding author Mondira Kundu, MD, PhD, St. Jude Department of Cell & Molecular Biology. “These different patterns can have dramatically different effects on how cells function.”
mtDNA mutations are not random passengers in cancer
To overcome this challenge, the team combined several techniques, including powerful computational tools, statistical analyses, bulk whole genome sequencing and single-cell studies. This approach allowed them to determine how much mitochondrial DNA was mutated in each cell, and when these changes happened in relation to cancer development. Surprisingly, the researchers found that some mitochondrial DNA mutations occur before a cell turns cancerous — and that these mutations are not always random. It appears that in some cases, cancer cells actively “select” for a mix of normal and mutated mitochondrial DNA.
“This approach allowed us to tell apart harmless ‘passenger’ mutations from those that may help cancer grow,” Kundu explained. “That’s something the field has struggled with until now.”
Kundu’s team took the analysis further by deploying a tool, called NetBID2, created by co-author Jiyang Yu, PhD, St. Jude Department of Computational Biology interim chair. With this tool, the researchers found evidence that mtDNA may contribute to therapy resistance. They discovered a mtDNA mutation linked to changes in pathways associated with resistance to glucocorticoids, a common therapy for acute lymphoblastic leukemia. Further analysis suggested that this type of mitochondrial mutation may make leukemia cells more likely to resist treatment.
While this research highlights the role mitochondrial DNA mutations might play in leukemia, the main achievement is the creation of a novel multidimensional approach to investigate mtDNA. Kundu is optimistic about the value of digging deeper into this overlooked feature of cancer growth.
“This work shows that mitochondrial DNA can influence both how leukemia starts and how it progresses,” said Kundu. “The next important step is to apply this approach to many more patient samples, so we can fully understand its impact.”
Discussion on Covid “Vaccination” Should Be Non-Controversial – Ok, I’ll start. It’s not safe, not effective, not tested, forced on people or they get fired, turbo cancer, Myocarditis….Oh and Ivermectin and Hydroxychloroquine cured it for about .10 a pill. How’s that?
Mapped: Median Rent Price by u.s. State – Don’t come from a blue state where your prices are higher because of what you voted for and then try to change it. It’s why the prices are lower in most of the Red states. I lived through this when I grew up in Florida. I heard, it was so much better in New York. Well, go back to NY. You’re in Florida now and it’s not the same. Fortunatly, I don’t live in either.
We’re told we get our mitochondria from our moms, and that’s true.
In humans, mitochondrial DNA is almost exclusively maternally inherited. Sperm mitochondria do enter the egg, but they’re typically tagged for destruction—marked and cleared by mitophagy so the embryo keeps mom’s mitochondrial line.
But even though mitochondrial DNA comes from mom, dad’s workouts before conception may still shape a child’s endurance capacity and metabolic health, not by passing on his mitochondria, but by sending tiny sperm microRNA messages that tune early embryonic gene regulation.
In a new study, exercising fathers produced offspring with greater endurance and more mitochondria, an effect that tracked to sperm small RNAs that suppress a “molecular brake” on PGC-1α, the classic mitochondrial biogenesis switch.
The findings reframe preconception health as a two-parent story—mom supplies the mitochondria, but dad’s training status can still program how those mitochondria are used.
Untrained offspring inherit their father’s fitness
For the study, male mice completed 8 weeks of progressive endurance exercise training on a treadmill, a program that successfully enhanced their fitness. Compared to their untrained peers, they were leaner, had higher bone mineral density, superior endurance, greater energy expenditure, increased mitochondrial abundance, more fatigue-resistance type I muscle fibers, and (at the molecular level), increased expression of PGC-1α—the master metabolic regulator.
This better fitness and endurance showed up in their offspring. When male mice trained before conception, their offspring (who never trained) ran longer and farther (with lower post-exercise lactate levels) than mice from sedentary fathers, and their leg muscles looked like those of trained mice, with more slow-twitch/oxidative fibers, higher mitochondrial enzyme activity, and visibly more mitochondria.
They also mirrored their fathers’ body composition, with higher lean mass, lower fat mass, and improved bone mineral density compared to offspring of sedentary fathers. Metabolically, endurance-trained offspring exhibited higher oxygen consumption and burned more calories throughout the day.
Put on a high-fat diet, offspring of exercising fathers had better blood sugar control than those of sedentary fathers. Skeletal muscle was pinpointed as the main driver. Their muscles pulled in more glucose, stored more glycogen, showed stronger insulin signaling, and had more of the glucose transporter GLUT4.
Endurance capacity (B and C) and energy expenditure (D) in offspring of sedentary (blue) and endurance-trained (red) male mice.
PGC-1α’s crucial role
A complementary experiment showed the same effect without any treadmill training.
Fathers engineered to overexpress PGC-1α—the muscle’s “fitness switch”—passed on endurance benefits even when the transgene wasn’t inherited. Offspring that did inherit the transgene had a 31% higher peak VO₂ than controls, and even the wild-type littermates (whose fathers overexpressed PGC-1α but who lacked the gene themselves) showed a 14% increase in peak VO₂. Even when pups did not inherit the genetic tweak, they still showed the endurance and mitochondrial advantages, set up through a non-genetic mechanism.
Small sperm RNAs carry the message
Researchers isolated RNA from the sperm of exercising fathers and injected it into normal embryos. This alone recreated the full package of fitness and metabolic benefits in otherwise standard offspring, who had a leaner body composition, better endurance, and more mitochondria in their muscle.
The tiny RNAs worked by dialing down an embryonic brake called NCoR1, a corepressor that acts as a brake on PGC-1α-driven mitochondrial biogenesis. Exercise and elevated PGC-1α in fathers produced a shared signature of altered sperm microRNAs, several of which target NCoR1.
Injecting just one of those microRNAs (miR-148a-3p) into standard embryos reduced embryonic NCoR1 and was enough to produce adult mice with higher endurance and more oxidative muscle.
Body weight (B) and glucose tolerance (C and D) in offspring from sedentary (blue) and endurance-trained (red) male mice fed a high-fat diet.
Fitness-forward genes are conserved in humansTo test whether this pathway shows up in people, the researchers compared trained and untrained men. The trained group had markedly higher aerobic capacity (VO₂max of ~63 vs. ~53), confirming a meaningful endurance phenotype before looking at sperm biology. They then profiled the same exercise-responsive sperm microRNAs highlighted in the mouse experiments. Of the ten miRNAs consistently elevated after paternal exercise or PGC-1α activation in mice, seven are conserved in humans and all of them were significantly higher in sperm from the trained men. Is that amount of microRNA enough to matter at fertilization? Maybe. The study estimated ~830 vs. ~2,779 copies per sperm in sedentary vs. exercised males. Prior work suggests ~100 copies per cell can repress targets—so these amounts are plausibly active during the earliest embryonic stages. In short: endurance training is associated with the same conserved sperm-miRNA pattern in humans and exercised mice, making it biologically plausible that a father’s training status before conception could influence early embryonic gene regulation (even though child outcomes weren’t measured in this study).
DOI: 10.1016/j.cmet.2025.09.003
The importance of parental exercise
Unsurprisingly, most of the research on parental habits and childhood health has focused on the role of the mother before and during pregnancy—her body weight, what she eats and drinks, and other lifestyle habits she engages in or avoids. That’s especially true when it comes to exercise. The role of the father, however, is a bit more hazy.
For moms, randomized controlled studies show that exercise during pregnancy reduces the risk of pregnancy complications (macrosomia, abnormal vaginal delivery, C-section) and lowers the odds of gestational diabetes, hypertension, and preeclampsia—which pose short- and long-term health risks for mother and newborn.[1][2] There’s also possibly autonomic and neurodevelopmental advantages, for example, better language and cognitive development in children at age 2 and 5 if their mothers exercised regularly.[3]
For dads, human evidence is limited to molecular-level studies such as the one discussed today—we don’t have much information on long-term outcomes after paternal exercise, even though the mechanistic plausibility is there.
But we do know that fitness can be passed down. VO2 max trainability (how much one can improve their fitness via training) is estimated to have 47% heritability, and even endurance performance measures like lactate threshold show significant parent-offspring resemblance—highly trainable and fit parents are likely to have fitter, highly trainable kids.[4][5] Part of this is environmental, but part is also genetic. It’s not just fitness either—parents (particularly fathers) who are highly active have children who are more likely to be highly physically active throughout childhood and into adulthood. While this might reflect modeled lifestyle habits rather than inheritance per se, there’s likely a genetic component at play too.
As a heart surgeon, one of my favorite mantras is “hit your protein goal.” That’s because many of the patients who walk into my office see enormous metabolic improvements just by swapping dietary carbs for protein.
But maybe you’ve seen research talking about the unhealthiness of high-protein diets. Will getting rid of carbs increase your risk of a heart attack? Or will the amino acids in meat trigger cardiovascular disease?
From a purely scientific standpoint, probably not.
But I’ll go through the research so you can decide for yourself.
What science says about protein and the heart
Let’s start with the studies sounding the alarm about getting ‘too much’ protein in your diet.
Another found that “high-protein diets increase cardiovascular risk by activating macrophage mTOR to suppress mitophagy.” In other words, that high protein intake could overstimulate certain immune cells, leading to artery damage and higher cardiovascular risk.
Here’s a quick breakdown of their hypotheses:
Eating a large amount of protein in one sitting raises amino acid levels in your blood.
Those amino acids collect in artery plaque, or the fatty buildups that encourage atherosclerosis.
Inside the plaque, amino acids activate a signaling pathway in immune cells called macrophages (specifically called the mTOR pathway).
When this happens, types of white blood cells called macrophages stop clearing out damaged parts of cells.
These damaged cells die off, which makes artery plaque more unstable. This means it could rupture and cause heart attacks or strokes.
So researchers concluded eating more than 0.8 grams of protein per kilogram of body weight could be harmful to your heart.
Now, before you start wondering if going vegan is your only option, I’d like to point out a few limitations.
Most studies don’t control for the type of protein consumed. After all, there’s a big difference between eating a grilled chicken breast and a 10-count chicken nugget meal from a fast food franchise. Food quality matters, especially with protein, although many studies neglect this or don’t define it explicitly in their results.
Many mechanistic studies use isolated amino acids such as leucine or protein powders to measure protein impacts. However, we know the body doesn’t process amino acids from a whole steak or lentils the same way it processes them from supplements. Leucine in these studies may not act the same way in whole, real foods, since fiber, fat, and other nutrients slow absorption and change digestive impacts.
Mice don’t develop heart disease the same way humans do, so what causes atherosclerosis in mice doesn’t always translate to people. Look back at that study hypothesizing a higher risk of atherosclerosis from high protein. That number was present in a cohort of mice, not people.
Increased signaling in immune cells isn’t the same as a greater number of heart attacks or plaque buildup in the body. As one study found: “protein ingestion has a negligible impact on whole-body amino acid oxidation.” Biological reactions may not always translate to risk.
For all these reasons, among many others, we lack concrete data to say high-protein diets are “bad” for the heart. High protein may actually be critical to those recovering from heart attacks or reclaiming metabolic health.
One study found that high-protein diets improve weight loss, reduce triglycerides, and improve HDL cholesterol, all of which are protective for the heart.
We also also know people lose muscle mass and bone density due to inactivity and inflammation after a heart attack. A higher protein intake can help maintain this lean body mass, which supports exercise tolerance and recovery moving forward.
This complements yet another study: higher protein intake after a heart attack may improve long-term patient prognosis. According to their analysis, heart attack patients eating high-quality protein had a much lower 10-year cardiovascular risk score compared to patients eating +50% less protein per week.
Why does research say two different things?
First, nutrition science is still quite young. It’s been less than 100 years since we isolated the first vitamin, after all. The science isn’t settled, and there’s still much to learn, so it shouldn’t come as a surprise that we’re still exploring new biomechanisms.
We also have to look at differences in terms and study structure. There’s a big difference between studying metabolically unwell young people versus metabolically healthy older adults, for example.
And don’t forget that N = 1. One person’s response to protein won’t be the same as someone else’s, especially within unique age, sex, or health cohorts.
But I can confidently say that the benefits of protein far outweigh any warning to the contrary, especially for those recovering from poor metabolic health.
What about all those other problems with protein?
Protein has become quite the target for misinformation. If you’re active on X, you likely know what I mean.
I can’t dispel all protein myths here, but I felt it was appropriate to cover a few topics.
First: most people actually underconsume protein, not overconsume it. Americans have a mean protein intake of 16%, which is less than half the max range of even US food pyramid RDVs.
And no, high protein isn’t bad for the kidneys. If you live with liver and kidney problems, then yes, you may need to plan your meals. But this applies only to a very small portion of the population.
When healthy, resistance-trained adults consume high-protein diets (think 3x higher than recommended daily values), there is no evidence of harmful side effects on kidneys and renal function. You can find details of that in this study and this one.
So please: don’t believe for one second that increasing your protein intake will do more harm than good. If you’re looking to repair, restore, or protect your metabolic health, a high-protein diet will be an incredibly powerful tool.
So will too much protein hurt your heart?
No, not at all. Especially not as part of a metabolically healthy lifestyle.
And if you’re at high metabolic risk, it might be worthwhile to increase your macros.
That means:
Eating more whole, real animal proteins. I recommend ruminant animals such as beef, venison, buffalo, and lamb, although chicken, turkey, and seafood are excellent choices. I talk through other options in my guide covering the proper way to set a protein goal.
More non-muscle proteins such as cheese, eggs, and milk. Despite what you may have heard, eating eggs won’t spike your LDL cholesterol and lead to heart disease.
Supplementing when necessary with convenient protein options. Uncured, less processed options such as meat snacks may be beneficial. You could also opt for protein powders, although I’d recommend those without high quantities of lead.
Following a high-protein diet for better heart health
High-protein diets aren’t a danger to your heart health. For the vast majority of people, it’s one of the best lifestyle changes you could make.
If you’re not sure how to get started, I’ve written quite a few guides. Learn more about using high-protein diets to support your heart health in the following resources:
Now we are allowing AI to create new viruses? Are we mad? What scientists at Stanford University are doing sounds like the plot to a really bad disaster movie. Viruses that are designed by AI are assembled by crazy researchers, and then those viruses start hunting down bacteria and reproducing. Needless to say, it doesn’t take much imagination to see where the rest of the movie would go. I realize that all of this sounds completely insane, but this is actually happening in real life. Our scientists really are assembling viruses that have been dreamed up by AI, and those viruses really are “capable of hunting down and killing strains of Escherichia coli”…
Scientists have created the first ever viruses designed by artificial intelligence (AI), and they’re capable of hunting down and killing strains of Escherichia coli (E. coli).
“This is the first time AI systems are able to write coherent genome-scale sequences,” says Brian Hie, a computational biologist at Stanford University, California. “The next step is AI-generated life,” says Hie, although his colleague Samuel King adds that “a lot of experimental advances need to occur in order to design an entire living organism”.
We are bringing viruses into existence that have never existed before.
I guess when AI gets smart enough to know that we can pull the plug, the robots will kill the humans. The story always ends that way. There is some stuff we should just leave alone
I see patterns and within the first couple of killings, I commented that it’s Trannies a lot who are on psycho meds and other drugs to try and make their bodies look like not what they were born as.
Unlike the first sentence below, I haven’t spent a lot of time on it because everyone else has. The only way it’s going to stop is to stop what’s making them kill.
Every kid has troubles growing up and cutting off your dick or your tits aren’t going to fix that. Life is hard, and apparently gets harder.
Maybe you spent time last week perusing X postings related to Charlie Kirk’s assassination. Aside from the many accolades, conservative influencers did fine jobs identifying left-wingers who not only celebrated Kirk’s assassination, but offered attaboys to Tyler Robinson, the triggerman. Some even called for more violence. If you didn’t have time earlier, scroll through the Libs of TikTok’s and the Vigilant Fox’s threads, for starters. You’ll get an eyeful. “Somebody had to do it” wasn’t an uncommon refrain. Who, this side of hell, delights in an act of murder?
What was striking was that many of the posts featured females. Was that the result of sampling biases? Not likely. It was self-promotion. Call it malignant feminist self-empowerment. Not that there aren’t Charlie Kirk haters among “progressive” males — his killer is an XY, after all, who lived with a trans — but left-of-center females dominated the posted videos. Why so?
There’s no point rehashing Kirk’s qualities or listing his achievements. Others who knew him have provided rich, poignant testimony to his stellar character and unshakable dedication to his faith and freedom. His very public record is testament enough.
If you sift through the haters’ postings, you’ll think they inhabit an alternative universe. Abundant public record be damned. For them, Kirk was an ogre, some mythical beast. He checked off every box that inflames the leftist mind. Homophobe, transphobe, this-phobe, that-phobe. They fictionalized Kirk. Damn reality, too!
Are the celebratory outpourings over an innocent man’s murder indictive of a sickness in our society? Yes, they are.
That sickness starts with an obsession — the obsession with self. “If it feels good, do it” was a 60s mantra that has sparked a decades-long deep dive into hedonism, regardless the blarney about “self-actualization.” The Me Generation ethos metastasized, spreading throughout the society.
I’m playing with the title and the concept, but I can cover more territory this way. When I want to pontificate, I’m more than happy to upset or make a lot of people happy.
I’m trying new things to keep it interesting. I’ll keep them brief, this isn’t the Drudge Report.
It’s worse than you think. The stats and link are at the bottom. Don’t say you weren’t warned.
“Doctors are being paid to vaccinate, not to evaluate,” Health Secretary Robert F. Kennedy Jr. said in a recent video.
“They’re pressured to follow the money, not the science.”
Doctors administer dozens of vaccines to many children in the United States. Adults are also advised to receive multiple shots.
Here’s what to know about vaccines and payments.
What Does the Literature Say?
A review of studies confirms that some doctors profit from vaccinating.
In a 2020 paper, researchers found when analyzing three years’ worth of vaccination claims for five Colorado clinics that reimbursements averaged 125 percent of costs, making administering vaccines “financially favorable across the practices.”
Another study found that various providers in North Carolina, when receiving the maximum payment for reimbursement from insurers or the government, profited from vaccinating patients. Even if they received the minimum payment, pediatric and family medicine practices still reported positive income, according to the 2019 study.
On the other hand, other doctors say the costs of administering certain vaccines to certain people exceed the vaccine payments.
In a survey of 34 pediatricians, for instance, more than half said they do not profit from vaccinating, according to a 2009 paper.
A number of practitioners have also said they face escalating costs associated with vaccination, such as staffing, leading them to stop or consider stopping providing vaccines to patients with private insurance.
Reimbursement for vaccinating patients varies depending on whether patients have private or public insurance. Under a program called Vaccines for Children, the government also provides vaccines to doctors for free. It does not pay for related costs, but doctors can charge an administration fee that the Centers for Disease Control and Prevention says “helps providers offset their costs of doing business,” with the maximum varying by state.
A nurse prepares to give a COVID-19 vaccine to a boy as his mother comforts him in Denver on Nov. 3, 2021. Michael Ciaglo/Getty Images
What About Those Bonuses?
Doctors can make extra money for vaccinating under incentive programs from insurers, as highlighted by Brian Hooker, a senior scientist with Children’s Health Defense—a group Kennedy chaired through 2023—and other witnesses during a hearing in July on vaccines held by Sen. Ron Johnson (R-Wis.).
“Some pediatricians can make upwards to a million or more a year just in those incentives,” Hooker said.
Asked for citations, Hooker pointed The Epoch Times to documents he collected from insurance companies that list available bonuses.
Links to those and other documents that outline incentives and are available online are provided below:
Blue Cross Blue Shield Blue Care Network of Michigan: $400 per child who receives a set of 24 or 25 vaccine doses on or before their second birthday.
Aetna Better Health of Louisiana: $10–$25 per member, depending on level of COVID-19 vaccination coverage practice-wide.
Molina Healthcare of Ohio: $100 incentive for COVID-19 vaccination.
Anthem Blue Cross and Blue Shield Medicaid: $50 per individual aged 6 months and older who received a COVID-19 vaccine by Dec. 31, 2022.
United Healthcare Community Plan of Michigan: Incentives for patients who receive the meningococcal, Tdap (tetanus, diphtheria, and pertussis), and HPV vaccines by their 13th birthday.
Meridian: Up to $120 per child who receives the 24 or 25 doses by their second birthday, or adolescents who received three certain doses by their 13th birthday, capped at $9,600 for each category.
BlueCross BlueShield of Illinois: $149 for each child, if 63 percent or more meet criteria, who received the 24 or 25 vaccine doses by the time they turn 2.
Central California Alliance for Health: Bonuses for children who receive at least 24 doses by the time they turn 2 and the three certain doses before they turn 13.
The sets of vaccines for which providers receive bonuses are recommended by the Centers for Disease Control and Prevention.
The government is killing them off as fast as they did in France with the Guillotine. What about that socialized healthcare that the celebtards were raving about?
According to a recent article in TheAtlantic, assisted suicide is now so popular in Canada that doctors cannot keep up with the demand. Appropriately titled Canada is Killing Itself, the article described how Medical Assistance in Dying (or MAiD), passed just 10 years ago, now accounts for about one in 20 deaths in Canada. That number is more than the total number of combined deaths from Alzheimer’s and diabetes, and it surpasses many countries where assisted dying has been legal for far longer. The shortage of “care” is not due to a lack of interest from medical professionals. Doctors are in fact flocking to join what the Atlantic article called “the world’s fastest-growing euthanasia regime.”
For example, Dr. Stefanie Green, a founder of the Canadian Association of MAiD Assessors and Providers, traded in her decades-long practice as a maternity doctor to end lives. Both kinds of medicine, she told The Atlantic, are “deliveries.” Some doctors have reported euthanizing hundreds of patients and yet, the demand exceeds the supply.
Despite what Canadian officials have claimed, there are no effective “safeguards.” A report last year in the New Atlantis noted hundreds of serious violations of regulations in just the Ontario province, and none have been reported to law enforcement. Although Ontario Chief Coroner Dirk Huyer boasted, “Every case is reported. Everybody has scrutiny on all these cases,” physician whistleblowers identified over 400 “issues with compliance.” These range from patients killed who were not capable of consent to communication breakdowns with pharmacists providing the deadly prescriptions. For example, only 61% of physicians notify pharmacists about the purpose of the euthanasia medications prior to dispensation, as required.
The Treasury Department has confirmed a national security and public safety disaster: Chinese money-laundering networks have pushed more than $312 billion in illicit transactions through U.S. financial institutions in recent years.
That money financed Mexican drug cartels, enabled human traffickers, and supported organized criminal networks that have left tens of thousands of Americans dead from fentanyl overdoses and other cartel-driven violence.
According to FINCEN.gov, financial institutions filed 1,675 BSA reports in the dataset indicating suspicious activity potentially involving human trafficking or human smuggling.
FINCEN.gov also discovered funds potentially associated with healthcare fraud, elder abuse, and suspicious gaming activity.
What makes these Chinese Money Laundering Networks (CMLNs) especially dangerous is their coordination with Mexico’s most violent cartels, including the Sinaloa and Jalisco New Generation organizations.
Mexico’s strict limits on U.S. dollar deposits force cartels to look abroad, while China’s own capital controls make moving money out of the country nearly impossible through legal channels.
Criminals found the perfect solution: CMLNs convert cartel drug profits in dollars into Chinese renminbi and then cycle those funds back into the U.S. banking system.
The cartels get clean money. China’s elites get access to American assets. And Americans pay the price in drug overdoses, gang violence, and financial corruption.
My wife is Scandinavian. I’ve heard 3 decades of shit from them about free education, free medical, and free money if you can’t work or are going to school, or basically, if you are alive, you can suck off the system. There are a lot of illegals and goat herders who are getting free money also. Someone is paying for it.
The problem I point out is that their 70% tax rate is paying for this.
The other problem is that almost everyone in her family who got an operation had to either have it redone or had results that would be malpractice were it not socialized medicine.
Not all of her country finishes high school. So much for the education.
Even they don’t believe it is free anymore. Their argument couldn’t hold water as soon as I asked a couple of questions about how the economics work. They can be insufferable so the less we talk, usually the better, for me at least. You can only listen to so much shit before it gets old and it got old for me decades ago.
Now This:
Europe’s free university model is often seen as a triumph of modern society. With no crushing tuition bills, minimal student debt, and a promise of equal access, it sounds ideal. In countries like Germany and France, students pay only a small administrative fee, typically between $200 and $500 a year, compared to the staggering tuition costs in the US or UK. Many also receive financial aid in the form of grants that don’t need to be repaid, or low-interest loans based on need.
But behind the promises of fairness and opportunity lies a system that too often feels rigid, overcrowded, and uninspiring.
For all its accessibility, the reality of navigating these institutions can leave students feeling like just another number in a giant, bureaucratic machine.
When education is available to everyone, universities become packed. Lecture halls overflow, and personal contact with professors becomes rare. In many European countries, it is normal to attend classes with hundreds of other students. There is little space for discussion, feedback, or even questions.
You sit, you take notes, you pass or fail. It feels more like an assembly line than a place for learning. And the numbers explain why. In 2022, the European Union had 18.8 million students, about 7 percent of its total population, enrolled in tertiary education. In the United States, about 19.1 million people were enrolled in college during the 2024–25 academic year. In addition to similar enrollment figures, both the EU and the US have made higher education widely accessible. In the EU, where tuition is often free or heavily subsidized, higher education has been expanded to accommodate the majority. As of 2022, 44 percent of EU citizens aged 25–34 had completed a tertiary degree, compared to 50 percent in the US.
The two systems differ in structure. What sets these systems apart is not the number of students, but how education is delivered. European universities tend to rely on large lectures, rigid course pathways, and limited institutional competition. The result is a model built for efficiency over individualization. US institutions, by contrast, operate in a competitive, decentralized environment with a wider range of academic structures, including smaller colleges and more flexible program design.
When higher education is scaled to serve nearly everyone, as in much of Europe, it risks trading depth for throughput and personalization for administrative convenience. It works, but at the cost of treating education less as a journey and more as a bureaucratic process.
This is posted at the same time as the post about Americans refusing the jab because they know it’s dangerous and it doesn’t work. I did it on purpose so read both.
Just so you know that the CDC is a bunch of CSMF who don’t have your health in their best interest. Here’s your tip of the day, keep the government out of your medical life as much as possible.
The U.S. Centers for Disease Control and Prevention is insisting people take MORE COVID shots this year, despite a long list of serious side effects that include cardiac arrest – or death.
The shots were introduced during the pandemic several years ago that circled the globe and killed millions.
They all were introduced under an “experimental” label as manufacturers wanted to start selling them before the ordinary testing procedures were done.
The medical establishment, including such high-profile personalities like Anthony Fauci, the adviser to Joe Biden on COVID who once insisted that arguing with him was arguing with “the science,” publicly rejected existing treatments that could, and did, help some people, ivermectin and hydroxychloroquine, because for the experimental products to be used there was a requirement that other treatments not be available.
Now comes this year’s advisory in which the CDC repeatedly demands people get the shots, without a single word about the potentially lethal side effects.
It shoots down the abortionist (liberal) argument that a pre-born baby is just a bunch of cells. It proves life begins at conception, or this couldn’t be true.
Via Freepik
On July 26, 2025, Thaddeus Daniel Pierce was born in Ohio from an embryo frozen for over 30 years, marking a record for the longest-frozen embryo leading to a live birth, as reported by MIT Technology Review.
Lindsey and Tim Pierce adopted the embryo through Nightlight Christian Adoptions’ Snowflakes program. The embryo, created in 1994, originated from biological mother Linda Archerd via IVF.
In the early 1990s, Archerd and her then-husband faced infertility for six years before turning to IVF, a then-emerging technology, according to the BBC.
They produced four embryos, with one implanted to become Archerd’s now-30-year-old daughter, who has a 10-year-old child. The remaining three were cryopreserved, with Archerd paying annual storage fees of about $1,000.
After her marriage ended and she reached menopause, Archerd, now 62, chose not to discard the embryos or donate them for research.
As a Christian, she opted for embryo adoption to have input on the adoptive parents. She specified preferences for a married, Caucasian, Christian couple in the US.
Lindsey Pierce, 35, and Tim Pierce, 34, had tried for seven years to conceive before exploring embryo adoption. They registered with the Snowflakes program, open to various embryo criteria.
Good, get that poison out of the system. It’s a death jab unless they learn to understand DNA. The last administration used it as a weapon instead of a cure. We’re not ready yet for this to be productized. Look at the excess deaths and turbo cancers because of the Covid jab
Health Secretary Robert F. Kennedy Jr. criticized mRNA vaccines in a video posted on his social media accountsImage: Allison Bailey/NurPhoto/picture alliance
The US government has decided to halt the funding of 22 projects focused on the development and manufacturing of mRNA-based vaccines that help fight respiratory diseases like COVID-19 and the flu.
The decision, announced by Health Secretary Robert F. Kennedy Jr., stemmed from his personal and unproven theories about the efficacy of vaccines and marks the latest attempt in a string of efforts that weave vaccine distrust into US health policy.
What did Kennedy say about the vaccines?
“We reviewed the science, listened to the experts, and acted,” Kennedy said in a statement.
The health department’s Biomedical Advanced Research and Development Authority (BARDA) is “terminating 22 mRNA vaccine development investments because the data show these vaccines fail to protect effectively against upper respiratory infections like COVID and flu,” he added.
In total, the halted projects are worth “nearly $500 million,” the Department of Health and Human Services (HHS) said.
According to a new study published last week in NPJ Vaccines, Japanese researchers engineered an entirely new strain of bird flu, combining the genetic material of two separate wild viruses to create what they call Vac-3: a pathogen that is “a reassortant virus between A/duck/Hokkaido/101/2004 (H5N3) and A/duck/Hokkaido/262/2004 (H6N1).”
This lab-built virus—A/duck/Hokkaido/Vac-3/2007 (H5N1)—was never observed in nature.
It was artificially assembled, grown in eggs, concentrated, and inactivated with formalin to become the whole-particle vaccine used in long-term testing on nonhuman primates.
The new study comes after NIH-funded researchers at the University of Georgia, Mount Sinai, and Texas Biomed were caught engineering lab-made H5N1 bird flu viruses—one of which killed 100% of exposed mammals—using synthetic DNA constructs and then deliberately infecting live dairy cows, all under the same $59 million federal contract that has also been tied to mammal-adapted, drug-resistant strain development.
Japan is also working with U.S. scientists on other projects to build lab-made horse-human influenza hybrids that replicate 100 times faster than natural strains using aborted fetal cells engineered with the cancer-linked SV40 virus, also under the banner of vaccine development.
All of these developments raise fears that another man-made pandemic is on the horizon, as Congress, the White House, the Department of Energy, the FBI, and the CIA have acknowledged that a lab-related incident involving gain-of-function research is most likely the origin of COVID-19.
A Louisiana woman is being accused of fraud by investigators who say she was running a multi-million-dollar empire involving several companies and bought a $100,000 Lamborghini but still claimed – and took – Medicaid benefits.
A report from Fox News explains Candace Taylor, 35, from Slidell, is facing felony counts, accused by Louisiana Attorney General Liz Murrill’s office of fraudulently taking Medicaid benefits.
That’s right. They can survive and are living beings at a time you think they don’t feel pain. How could you be so cruel? FWIW, I had a fight at work with Alise and was so taken aback that a female who had given birth in the past year wanted to kill babies because she was a liberal.
A can of soda weighs in at an arm-breaking 12 ounces. A large slice of pizza, maybe inflicting only a sprain, weighs around 8 ounces.
Nash Keen, when he was born 19 weeks premature, weighed in right between those, at 10 ounces.
And now he’s a smiling, bouncing, engaging baby boy of one year old.
The Christian Institute in the United Kingdom marked the birthday for Keen, born to an Iowa family at 21 weeks, one day earlier than the previous Guinness World Record holder.
“He spent the first six months in the neonatal intensive care unit (NICU) at Stead Family Children’s Hospital in Iowa, but is now home,,” the institute reported.
“His mum Mollie thought they would lose him,” the report said.
“I had to take it one day at a time. I focused on the small victories and leaned hard on my support system,” she explained.
“Being in the NICU as long as he was, you’d think that he would be, you know, more fragile and stuff. And he’s not. He’s a very determined, curious little boy, and he’s just all smiles all the time,” she continued.
As fireworks light up skies across America this Fourth of July, George Zambelli, owner of Zambelli Fireworks, urged people on Newsmax on Friday to leave the explosions to the professionals — and to never handle fireworks while under the influence of alcohol.
Zambelli has seen nearly everything in his decadeslong career running one of the nation’s largest fireworks companies. But as Independence Day celebrations get underway, he’s sounding a familiar alarm: Fireworks and alcohol do not mix.
Who would have thought that those 2 don’t mix well
What was once dismissed as a “conspiracy theory” now has hard data behind it.
A new peer-reviewed study out of the Czech Republic has uncovered a disturbing trend: in 2022, women vaccinated against COVID-19 had 33% FEWER successful conceptions per 1,000 women compared to those who were unvaccinated.
A “successful conception” means a pregnancy that led to a live birth nine months later.
The study wasn’t small. It analyzed data from 1.3 million women aged 18 to 39.
Here’s what the numbers reveal, and what it could mean for humanity.
By 2022, a stark difference was clear.
The vaccinated cohort averaged around 4 successful conceptions per 1,000 women per month.
That’s a staggering 33% LESS than the 6 per 1,000 seen in the unvaccinated group.
This means that for every 2 vaccinated women who successfully conceived and delivered a baby, 3 unvaccinated women did the same.
In 2022, unvaccinated women were 1.5 times MORE likely to have a successful conception.
Again, that’s a conception that led to a live birth nine months later.
Prince William’s longtime friend, Sunjay Kapur, has died at age 53 after swallowing a bee, which triggered a fatal heart attack.
The billionaire businessman and chairman of global car parts giant Sona Comstar collapsed during a polo match in England on Thursday, the Mirror reports.
Kapur, who was the former husband of Bollywood superstar Karisma Kapoor, was stung by a bee on the mouth, which subsequently triggered anaphylactic shock that caused his heart to stop, the outlet added
I already gave up on the flu shot after the Covid lies. They didn’t get me on that one either. I wonder how much longer we can go to avoid people who are purposely trying to hurt you.
Hippocrates, are you there?
Alex Jones discusses Director of National Intelligence Tulsi Gabbard’s bombshell release exposing how the Biden administration secretly labeled millions of lockdown and mandate skeptics as “domestic violent extremists,” and breaks down how the FDA has long been aware of flu shot deaths.
BREAKING: The FDA Has Known For At Least 20 Years That Flu Shots Cause A Massive Increase In Flu Cases & Lead To Early Death
Meanwhile, Tulsi Gabbard Has Released Documents Proving That The Biden Admin Secretly Listed Millions Of Ameicans Who Questioned The Tyrannical COVID… pic.twitter.com/rFixHcauNq
Life expectancy at birth measures the average number of years that a newborn could expect to live, if they were subject to the age-specific mortality rates of a given period.
ℹ️ This number visualized is an average between men and women. For extra context, women have higher life expectancies than men in nearly every country in the world.
Ranked: Countries Where People Live the Longest
The micronation of Monaco has the highest average life expectancy in the world. A baby born in the country in 2025 can expect to live to 87 years old.
Former Harvard Morgue Manager Pleads Guilty To Trafficking Stolen Human Remains
The United States Attorney’s Office for the Middle District of Pennsylvania announced that Cedric Lodge, age 57, of Goffstown, New Hampshire, pled guilty yesterday before Chief United States District Judge Matthew W. Brann to interstate transport of stolen human remains.
According to Acting United States Attorney John Gurganus, Lodge admitted that, from 2018 through at least March 2020, he participated in the sale and interstate transport of human remains stolen from Harvard Medical School morgue, located in Boston, Massachusetts. Lodge, who was then employed as the manager of the Harvard Medical School Morgue, removed human remains, including organs, brains, skin, hands, faces, dissected heads, and other parts, from donated cadavers after they had been used for research and teaching purposes but before they could be disposed of according to the anatomical gift donation agreement between the donor and the school. Lodge took the remains without the knowledge or permission of his employer, the donor, or the donor’s family, and transport the remains to his home in New Hampshire. After he and his wife Denise Lodge sold the remains, they would ship the remains to the buyers in other states or the buyer would take possession directly and transport the remains themselves. Remains stolen and sold by Lodge were transported from the morgue in Boston to locations in Salem, Massachusetts, New Hampshire, and Pennsylvania.
Lodge admitted to having sold remains to Joshua Taylor and Andrew Ensanian, among others. Many of the remains purchased from Lodge were resold for a profit, including to Jeremy Pauley, who previously entered a guilty plea to conspiracy and interstate transportation of stolen human remains.
Several other defendants have previously entered guilty pleas in related cases, including Lodge’s wife, Denise Lodge, Joshua Taylor, Andrew Ensanian, Matthew Lampi, and Angelo Pereyra. Lampi was sentenced to 15 months in prison and Pereyra was sentenced to 18 months. Denise Lodge and Joshua Taylor are still awaiting sentencing. Additionally, Candace Chapman-Scott, who stole remains from an Arkansas crematorium where she was employed and sold them to Pauley in Pennsylvania, entered a plea of guilty in Arkansas federal court and was sentenced to 15 years in prison.
So now we learn not only that Joe Biden has Stage Five prostate cancer, but that starting in February 2021, the POC/LGBTQ committee that was operating Biden like a Muppet concealed, then downplayed the risk of heart disease from the COVID vaccines.
It’s funny how we find out all this dirt, within 48 hours after the committee’s announcement about Joe’s cancer. Because he’s got a few months to live, he’s now officially the “Fall Guy.”
Everything bad can be blamed on him, if it can’t be blamed on Trump. All the Muppeteer committee members can pretend they’re innocent and resume their White House and Cabinet posts on January 20, 2029 if the Democrat party Deep State (DPDS) steals another presidential election.
So now we learn not only that Joe Biden has Stage Five prostate cancer, but that starting in February 2021, the POC/LGBTQ committee that was operating Biden like a Muppet concealed, then downplayed the risk of heart disease from the COVID vaccines.
It’s funny how we find out all this dirt, within 48 hours after the committee’s announcement about Joe’s cancer. Because he’s got a few months to live, he’s now officially the “Fall Guy.”
Everything bad can be blamed on him, if it can’t be blamed on Trump. All the Muppeteer committee members can pretend they’re innocent and resume their White House and Cabinet posts on January 20, 2029 if the Democrat party Deep State (DPDS) steals another presidential election.
According to the report from the Senate Permanent Subcommittee on Investigations, officials knew as early as February 2021 that the vaccines were associated with myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the thin sac surrounding the heart). Still, they waited to warn the public until June as they pushed the vaccine on Americans.
The report concludes that U.S. health officials “knew about the risks of myocarditis,” “downplayed the health concern,” and deliberately “delayed informing the public about the risk.”
Sen. Ron Johnson (R-WI), who chairs the committee and will lead a hearing on it later this afternoon, told The Daily Wire that Biden officials delayed reporting the side effects because they were concerned about “vaccine hesitancy.”
“But in being concerned about that, they violated the inviolable principle of informed consent,” Johnson said.
Here is the full subcommittee report. This report never would have been prepared if Democrats had kept control of the Senate last fall. The Subcommittee on Investigations would have been launching new bogus investigations into Team Trump instead.
Spearheaded by Dr. Anthony Fauci, the official diktat of the DPDS was that the vaccines were “safe and effective.” They knew better. The Israelis had started distributing Pfizer vaccines several weeks before we did. So they knew that vaccinated patients were getting myocarditis with alarming frequency, months before we did. They were warning Joe’s Muppeteer committee, but that committee wasn’t passing on this warning to the American people.
This is another one of Fauci’s many crimes against humanity, the most evil being his funding of gain-of-function research at the Wuhan Institute of Virology, using our tax dollars. That’s how COVID was unleashed upon the world, causing the deaths of 2 million people worldwide, including a million Americans.
Very few government figures in recent history — Hitler, Stalin, Chairman Mao and Pol Pot, for example — have killed more of their own countries’ people.
I was almost one of them. I spent a month in the hospital, including 72 hours comatose on a ventilator. Then I had to learn how to walk again, because I’d spent so much time on my back in bed. This was very difficult at my age.
Millions of Americans, and millions more around the world, suffered terribly from this disease without dying. Thank you, Dr. Fauci. Your blanket pre-emptive pardon by the Muppeteer committee’s Autopen evidently shields you from civil liability as well. How convenient.
1 This one is for my wife’s niece in Denmark who thinks that Liz is the Bomb. Oh, she bombed ok. I count on anything Marian says to be wrong and the opposite of what the US should really do.
A couple from the UK has signed up to die together in the Sarco “suicide pod” in Switzerland, and their deaths will allegedly be filmed.
Peter Scott (86) and Christine Scott (80) contacted the assisted suicide group “The Last Resort” last year regarding the Sarco machine because they wanted to commit suicide together after Christine received a diagnosis of vascular dementia — dementia caused by reduced blood flow to the brain.
But it wasn’t the diagnosis that worried them; what they fear is that neither of them will receive prompt treatment for their health conditions through the National Health Service (NHS).
“The chances of getting prompt NHS treatment for the ailments of old age seem pretty remote, so you end up trapped by infirmity and pain,” said Peter.
He told News.com.au, “We have had long, happy, healthy, fulfilled lives but here we are old and it does not do nice things to you. The idea of watching the slow degradation of Chris’s mental abilities in parallel to my physical decline is horrific to me.”
Rather than live out their lives, the couple will enter the Sarco pod — a device that, at the push of a button, will release nitrogen into the air, reducing the oxygen. They will die from hypoxia. According to Inspire, their deaths will be “filmed and provided to a coroner as evidence, setting a historic precedent in the field of assisted dying.”
All the reason you want right there on why state run (or socialist) healthcare is not our friend and is a recipe for death, if by incompetence as much as intention
Michigan Rep. Shri Thanedar isn’t the first Democrat to file quixotic, attention-grabbing articles of impeachment against President Donald Trump on entirely specious grounds.
He break new ground, however, in being the first known mass serial animal abuser ever to do it. Take that, Al Green!
As the HuffPost reported in 2018, when Thanedar was a Michigan gubernatorial candidate, AniClin Preclinical Services was forced to close after its parent company went under. When it did, roughly 170 dogs and monkeys had to be rescued from the lab his company ran after they were left to rot inside the facility.
From a USA Today report about the group that rescued the abandoned beagles at the facility:
There’s more here, but I couldn’t read it all because I can’t take cruelty to animals. I take a dim view of humans that can do this to animals. Pricks.
Top US virologist Ralph Baric engineered the Covid-19 virus SARS-CoV-2 in his lab at the University of North Carolina as part of his work in connection with the 2018 DEFUSE funding proposal. That’s the story that’s been going round the internet for some months now (and not just in alternative media) and it all looks very damning for Baric and those connected with his research.
Details of the DEFUSE project were first leaked by Major Joseph Murphy, an employee of US military research agency DARPA, in the summer of 2021 and further details of earlier drafts have come to light this month thanks to public record requests from U.S. Right to Know (USRTK).
In DEFUSE, Baric proposed to create a virus that was, to most intents and purposes, SARS-CoV-2. The proposal included inserting a furin cleavage site into a coronavirus spike protein, an order for the restrictive enzyme BsmBI, the search for a binding domain that would infect ACE2 human receptors and a requirement for a viral genome around 25% different to SARS.
The SARS-CoV-2 virus contains a furin cleavage site in its spike protein, its genome includes the restrictive enzyme BsmBI, it has a receptor binding domain finely tuned to infect the ACE2 human receptor and its genome is around 25% different to SARS. A number of virologists have said that such features make SARS-CoV-2 a smoking gun for an engineered virus.
Baric obtained a patent for such novel viruses in 2018, just as he was putting DEFUSE together. In DEFUSE he proposed to infect wild Chinese bats with his newly patented viruses.
A groundbreaking study reveals that women using mifepristone, the abortion pill, face a staggering 22 times higher risk of life-threatening complications than claimed by the FDA and Danco Laboratories, the manufacturer of Mifeprex. This challenges the narrative from abortion advocates and corporate media that the pill, responsible for over half of U.S. abortions, is “safe and effective.”
Conducted by Ethics and Public Policy Center President Ryan Anderson and Director of Data Analysis Jamie Bryan Hall, the study is the largest known analysis of abortion pill outcomes. It examined insurance claims from Medicaid, TRICARE, Medicare, the Department of Veterans Affairs, and private insurers, covering 865,727 mifepristone prescriptions dispensed to 692,873 women between 2017 and 2023.
The findings highlight a significant gap between reported and actual risks, raising urgent questions about the safety of mifepristone. As the debate over abortion access intensifies, this data could reshape public policy and medical guidelines surrounding the use of abortion pills.
Thefederalist.com reports: Approximately 10.9 percent of those claims, or 94,605 chemical abortions, involved potentially life-threatening “serious adverse events” such as emergency room visits, hemorrhage, sepsis, infection, and/or follow-up surgeries for the women who had downed the abortion drug within the last 45 days.
They died with Covid, but not from it, but it didn’t fit the narrative.
The following is from Children’s Health Defense.
A new peer-reviewed study published in Scientific Reports found that nearly half of the deaths labeled as “COVID-19” in seven hospitals in Athens, Greece, were not caused by the virus. The study reviewed 530 deaths from January to August 2022 and found that only 25.1% were directly due to COVID-19.
In another 29.6% of cases, COVID-19 contributed to the outcome—but a full 45.3% of patients died from unrelated causes while simply testing positive at the time of death.
A clinical review revealed major inconsistencies between official death certificates and patient case histories:
Of 204 certificates listing COVID-19 as the direct cause of death, only 64.7% were confirmed.
Of 324 cases listing COVID-19 as a contributing factor, only 26.5% were confirmed after review.
The study also found:
More than half of patients who died from COVID-19, where vaccine status was known, were vaccinated.
Of those, 65.8% had received a booster, according to CHD’s Karl Jablonowski.
Inaccuracies on death certificates contributed to significant overcounts.
Hospital-acquired COVID infections were frequently misclassified as primary causes of death—especially among younger patients.
Younger patients who died with COVID-19 were more likely to have serious existing illnesses like organ failure or cancer.
Older patients who died from COVID-19 were more likely to receive oxygen or COVID-specific treatments like remdesivir.
Patients infectedduring their hospital stay were 130% more likely to be misclassified as having died from COVID-19.
“That the official reporting of death rates is that inflated, that far into the pandemic, strongly suggests the over-reporting was intentional.” — Dr. Clayton J. Baker, Internal medicine physician
Researchers noted that Greece’s official policy classified any patient who tested positive at the time of death as a COVID death—regardless of clinical findings. Experts say similar policies were used across Western nations.
“There was a financial desire to make a lot of money from rapidly developed mRNA vaccines and to set a precedent for this in the future. As infections from SARS-CoV-2 virus were generally quite mild, it was necessary to scare people into thinking COVID-19 was far more severe, and far more prevalent, than it actually was.” — Dr. David Bell, Public health physician, Biotech consultant
The study relied on full clinical audits, physician interviews, and patient chart reviews—offering a more accurate analysis than studies based on administrative codes. Researchers selected the Omicron wave for its lower severity, where death misclassification was easier to detect.
Karl Jablonowski said the damage extended far beyond recordkeeping. He said the study’s results show that public health decisions during the COVID-19 pandemic were guided by fear instead of scientific or medical criteria.
“Regardless of what the intention was behind the over-exaggeration of COVID-19 deaths, the consequences led us down the wrong path … We isolated with closed doors and mask coverings. We administered experimental drugs and experimental vaccines. Our hospitals became places of harm.” — Karl Jablonowski
More bad news from the Covid Jab. So much for safe and effective.
An alarming study involving over 2 million participants has confirmed that Covid mRNA “vaccines” cause devastating long-term harm by sabotaging people’s immune systems.
The major study found that mRNA injections attack thyroid function, making recipients vulnerable to deadly diseases such as cancer.
The group of leading researchers behind the study is sounding the alarm with an urgent warning about the long-term effects of Covid mRNA injections on thyroid health.
The study was led by renowned neurology and radiology experts Drs. Kai-Lun Cheng and Hsiang-Lin Lee, both with Chung Shan Medical University in Taichung, Taiwan.
The groundbreaking study was published by Oxford University Press in the Journal of Clinical Endocrinology & Metabolism.
During the study, which included over 2.3 million patients, the researchers used the TriNetX federated data platform, which aggregates real-world electronic medical records.
The researchers analyzed a staggering 2,333,496 patients through a retrospective cohort study spanning two years.
Half of the group was vaccinated for Covid and the other half was unvaccinated.
The study found that Covid “vaccines” influence the incidence of thyroid dysfunction, including subacute thyroiditis, hyperthyroidism, and hypothyroidism.
There will be a number of Covid posts today, but it will show they knew, they knew it would cause damage and they did it anyway. Ivermectin and Hydroxychloroquine prevented and cured Covid-19.
1. So more and more truth is coming out about Covid and the vaxx. At this point, people aren’t taking the mRNA shots anymore, so… not a help. Unless of course, it leads to accountability and the restoration of our individual rights to refuse anything even remotely like this in the future. Or more importantly, if people energize their gonads and take back their God given rights and do not permit anything like this to happen in the future. Which we almost certainly won’t do.
“The Proximal Origin of SARS-CoV-2” publication — which was used repeatedly by public health officials and the media to discredit the lab leak theory — was prompted by Dr. Fauci to push the preferred narrative that COVID-19 originated naturally.
Breast cancer diagnoses have skyrocketed by an alarming 1000% among American women who received Covid mRNA “vaccines.”
Data shows that cases have surged dramatically since Covid injections were rolled out for public use in early 2021, particularly among younger women.
Breast cancer cases have skyrocketed in Americans under 45 years old who received the “vaccines.”
From 2019 to 2021, there were approximately 26,000 recorded cases of breast cancer per year.
However, that figure spiked in 2022 and then surged dramatically in 2023 to unprecedented levels.
In 2023, a shocking 297,000 breast cancer cases were recorded, marking a staggering 1042.3% spike in just five years.
The rise in breast cancer cases coincides with a high percentage (90%) of American women receiving at least one dose of a Covid mRNA “vaccine.”
Natural health advocates argue that the increase in cancer cases, particularly aggressive and late-stage cancers among young individuals, is directly linked to the administration of COVID-19 vaccines.
The United States spends more on health care than any similarly large and wealthy country. However, in 2023, Americans had a life expectancy of 78.4 years, compared to an average of 82.5 among peer countries. This chart collection examines deaths in the U.S. and comparable countries through 2021, by age group and cause, to highlight factors that contribute to this life expectancy gap. The countries included in the comparison are Australia, Austria, Belgium, Canada, France, Germany, Japan, Netherlands, Sweden, Switzerland, and the United Kingdom.
The U.S.’s premature death rate (408 deaths per 100,000 people under age 70) in 2021 was almost twice the average of these similarly large and wealthy countries (228 deaths). About a third (32%) of the difference in premature death between the U.S. and similar countries is due to deaths from cardiovascular diseases, chronic respiratory diseases and chronic kidney diseases (which, combined, caused 105 deaths per 100,000 population under 70 in the U.S. in 2021). Additionally, in 2021, COVID-19 made up 24% of the difference in premature death rates between the U.S. and peer nations, killing 64 Americans out of every 100,000 under 70.
Another 12% of the difference between the U.S. and its peers’ premature death rates is due to substance use, which caused 29 deaths per 100,000 people under age 70 in the U.S. in 2021. For the purposes of this analysis, substance use deaths are defined as deaths occurring as a direct result of consumption of alcohol or illicit drugs, excluding any deaths from chronic diseases and organ damage caused by long-term use.
Deaths at younger ages bring down life expectancy more than deaths among older age groups. In the younger adult age group (15- to 49-year-olds), the difference in death rate between the U.S. and peer countries is largely driven by more deaths due to chronic diseases, COVID-19, and substance use. Among 15 to 49-year-olds, the U.S. death rate was 2.5 times that of comparable countries (192 vs. 76 per 100,000).
The charts below illustrate how among the under-70 population, the U.S. diabetes death rate is about 2.5 times that of comparable countries, the liver disease death rate is 1.6 times as high, and kidney disease death rate is 3.8 times as high. Additionally, the U.S. substance use death rate is four times that of comparable countries in the under-70 population, and the homicide death rate is nearly 8 times the average of peer nations.
I am beginning to feel intense pity for the regular citizens of the United Kingdom (UK).
Their leader is the absolutely horrendous Keir Starmer. Citizens can be tossed into jail for social media posts. Their electricity prices are soaring due to their leader’s green energy schemes.
Now there is another challenge that can be added to the list: Doctors in the UK are reporting a concerning increase in cases of necrotizing fasciitis of the vulva — a rare but extremely aggressive bacterial infection often called “flesh-eating disease.” This infection destroys soft tissue rapidly and can become fatal within hours if not treated promptly.
In a new case report published April 8 in the journal BMJ Case Reports, U.K. doctors describe three patients who were found to have necrotizing fasciitis of the vulva. The vulva includes the external female genitalia, such as the labia majora and labia minora, for example.
“Necrotizing fasciitis (NF), also known as flesh-eating disease, can arise when certain bacteria enter the skin through a wound — a cut, abrasion, burn, surgical wound, or even an insect bite,” Bill Sullivan, a professor of microbiology and immunology at Indiana University, who was not involved in the case report, told Live Science in an email. “NF can occur anywhere skin or tissue is breached, including genitalia.”
In necrotizing fasciitis, bacteria infiltrate the fascia, which is the connective tissue surrounding muscles, nerves, fat and blood vessels. The infection rapidly causes soft tissues to die, or “necrotize,” and spreads through the body very quickly.
A recent report from Shrewsbury and Telford Hospital NHS Trust detailed three women hospitalized with vulvar necrotizing fasciitis; one died less than 28 hours after diagnosis despite emergency surgery and intensive care.
In two of the cases, the women were diagnosed with vulvar necrotizing fasciitis in the emergency room. In the third, the woman developed it as a complication from an infected surgical wound.
One woman had seen a doctor five days earlier after noticing a spot on her mons pubis, and was prescribed antibiotics. But the treatment failed to clear the infection, and by the time she was hospitalized, the infection had spread throughout her labia majora, lower abdomen, and left hip. Despite surgical removal of her infected and necrotic tissue (also known as debridement) and intensive care support, the woman died of sepsis just 28 hours after her diagnosis.
The other two women survived their ordeal, though not without serious difficulty. Both needed “extensive surgical debridement” and one woman underwent three separate surgeries to remove tissue, which later required reconstructive surgery.
The hospital treated 20 cases between 2022 and 2024, surpassing the total number seen in the previous decade, indicating a concerning rise. Similar increases are being reported in other parts of Europe and the US, with invasive group A Streptococcus (the most common cause) infections doubling in the US between 2013 and 2022.
The number of invasive group A strep infections more than doubled from 2013 to 2022, according to a study from the Centers for Disease Control and Prevention published Monday in the Journal of the American Medical Association. Prior to that, rates of invasive strep had been stable for 17 years.
Invasive group A strep occurs when bacteria spread to areas of the body that are normally germ-free, such as the lungs or bloodstream. The same type of bacteria, group A streptococcus, is responsible for strep throat — a far milder infection.
Invasive strep can trigger necrotizing fasciitis, a soft tissue infection also known as flesh-eating disease, or streptococcal toxic shock syndrome, an immune reaction akin to sepsis that can lead to organ failure.
Girls, you need to learn how to keep that thing clean or we aren’t going to be able to service it.
The study documents the outcomes of 99 million people after they received Covid mRNA injections.
During the study, the researchers examined the official government data from eight countries.
Participants in the study included 99,068,901 Covid-vaccinated individuals.
The study has concluded that the injections are responsible for the global surge in sudden deaths and life-threatening illnesses.
The researchers found that staggering numbers of vaccinated people suffered serious complications such as heart failure, blood clots, strokes, brain disorders, and severely weakened immune systems.
Many of those tracked by the peer-reviewed study also died suddenly and unexpectedly.
The research was conducted by the Global Vaccine Data Network in New Zealand.
The study’s paper was published in the prestigious, world-renowned Vaccine journal.
Over the past three years, the study has documented the outcomes for 99 million people who were given Covid shots.
The most common serious medical side effects have been blood clots and myocarditis, both of which can be fatal.
Myocarditis is the inflammation of the heart muscle (myocardium), according to the Mayo Clinic.
The inflammation reduces the heart’s ability to pump blood.
The condition weakens the heart so that the rest of the body doesn’t get enough blood.
Clots can form in the heart, leading to a stroke or sudden cardiac arrest.
Now, after studying almost 100 million vaccinated people, the new study has confirmed that “the shots from pharma giants, including Pfizer, Moderna, and AstraZeneca have been associated with rare occurrences of heart, brain, and blood disorders.”
Participants from eight different countries were monitored for upticks in 13 medical conditions.
The study revealed that besides a slight increase in neurological issues, the vaccines were also associated with dangerous blood and heart-related medical conditions.
The researchers discovered soaring numbers of people suffering from myocarditis after doses of Pfizer-BioNTech’s and Moderna’s mRNA shots.
The study showed those getting AstraZeneca’s viral-vector shot had a 6.9-fold increased chance of pericarditis, an inflammation of the cardiac muscle.
The lead author of the study’s paper is Kristýna Faksová of the Department of Epidemiology Research at the Statens Serum Institute in Copenhagen, Denmark.
The younger half of Gen Z had their high school and college years wrecked by the Left’s lockdowns. Conservatives fought to reopen, to restore freedom, and to end the overreach.
Who would have thought it would have been Gen Z. X, Y and Millennials were idiots. I thought it was a trend. Maybe they can take over quicker, like I hope Prince William gets to be King soon so we don’t have to put up with King Chuckles the clown in the UK for very long.
An “alarming” new study has found that Covid mRNA “vaccines” triggered serious neuropsychiatric conditions, causing suicidal thoughts, violent behavior, and homicidal ideation to skyrocket.
The study also found massive surges in brain injury, cerebral hemorrhage, brain clots, and dementia among those who received the injections.
In total, the study identifies 86 serious neuropsychiatric safety signals linked to Covid shots.
The study was conducted by a team of leading American researchers, including Dr. Drew Pinsky and renowned cardiologist Dr. Peter McCullough.
The findings of their study were published in the journal PrePrints.
They analyzed data from the U.S. Centers for Disease Control and Prevention’s (CDC) Vaccine Adverse Event Reporting System (VAERS).
The period analyzed was from January 1990 through December 2024.
The researchers found that safety thresholds outlined by the CDC and Food and Drug Administration (FDA) were breached at unprecedented levels.
During the study, the researchers compared Covid mRNA “vaccines” to flu shot
mRNA vaccination causes long-term changes in a crucial part of our chromosomes — changes previously linked to inflammatory and autoimmune diseases and cancers including leukemia and brain tumors.
The finding came in a peer-reviewed paper from German researchers last week. The discovery might help explain post-mRNA jab “inflammatory diseases which occur in… [some] vaccinated individuals,” the researchers wrote.
In a discussion with outside reviewers that was published along with the paper, the researchers suggested the changes they found are “very likely” occurring in bone marrow cells, the source of all blood cells. Their finding comes as other researchers report rising deaths from leukemia – a blood cancer – in very highly vaccinated Japan.
In the paper, published in the journal Molecular Systems Biology on March 25, the German researchers examined changes in the chromosomes of macrophages in people who had received mRNA Covid shots.
Macrophages are immune cells that circulate in the blood and attack and destroy foreign invaders like viruses and bacteria. The scientists found alterations in a crucial part of the macrophage chromosome called the histone.
Genetic scientists compare histones to drums around which cables of DNA are wrapped. Unlike DNA itself, the histones do not contain actual genetic information, but they provide the structure for it.
As a result, histones play a crucial role in processing genetic material. When they are bunched closely together, the DNA they hold is hard to access, so the cellular machinery that uses DNA to make proteins cannot do so. When histones are more widely separated, cells will process, or transcribe, DNA more actively — potentially leading to tumor growth.
—
The specific change the researchers found is called “histone 3 lysine 27 acetylation,” abbreviated to H3K27ac. The H3K27ac change is known to be found in several different types of cancer and has attracted increasing scientific attention.
In February, Chinese researchers published a review on it, suggesting that it had “emerging potential as a therapeutic target in cancer.” The paper examined “the genetic mutation and epigenetic mechanisms by which H3K27ac might contribute to various types of cancer… [and] future directions for cancer treatment that might involve targeting H3K27ac.”’
Last fall, researchers in Poland offered a similar overview. “Histone acetylation… regulates gene expression [and] is associated with cancer initiation, development and progression,” they wrote. They specifically noted that the H3K27ac change had been found in leukemia and other cancers, including gliomas, a deadly form of brain cancer.
In their paper last week, the German researchers found the H3K27ac alterations occurred broadly across many chromosomal regions. In addition, they found the changes when they examined macrophages several months after the shots, even though macrophages typically die in one to two weeks.
“We were able to demonstrate that SARS-CoV-2 mRNA vaccination establishes extensive and persistent H3K27ac at promoters
[a specific region on the chromosome that encourages DNA transcription]
of short-lived macrophages,” they wrote in the paper, which was titled “Persistent epigenetic memory of SARS-CoV-2 mRNA vaccination in monocyte-derived macrophages.”
That fact suggests that similar changes may be occurring in longer-lived “monocytes,” which produce macrophages, the researchers wrote.
“The risk of integration of synthetic mRNA-based gene therapies and/or associated DNA fragment adulterants into the human genome of either somatic or germ cells are uncharacterized,” the legislation explains, adding that any germline integration “creates risk of random human genomic modifications being passed on to the next generation of Americans.”
South Carolina lawmakers have introduced a bill that would ban healthcare professionals from administering synthetic mRNA-based gene therapies, including COVID-19 vaccines, citing contamination, long-term safety concerns, and the risk of genetic damage to future generations.
Dr. Mary Talley Bowden, whose groundbreaking lawsuit forced the FDA to remove its anti-ivermectin social media posts in March 2024, celebrated the move.
“Add South Carolina to the list of states calling for an end to Covid mRNA shots,” she wrote in an X post.
HB 4262, introduced March 27, 2025, by Reps. Magnuson, Rankin, Edgerton, Duncan, Kilmartin, Cromer, and more than a dozen other co-sponsors, would amend the South Carolina Code to prohibit the use of certain mRNA products and impose strict penalties on violators.
“Synthetic messenger ribonucleic acid (mRNA)-based gene therapies, such as the COVID-19 vaccine, have caused substantial numbers of deaths, disabilities, and a wide range of serious adverse events,” the bill states.
The bill affirms mRNA-based products are “contaminated with DNA fragments, metallic particles, and other undisclosed and/or otherwise poorly characterized adulterants.”
It warns that no long-term studies have been completed on shedding, fertility, teratogenicity, mutagenicity, or cancer risk.
“The risk of integration of synthetic mRNA-based gene therapies and/or associated DNA fragment adulterants into the human genome of either somatic or germ cells are uncharacterized,” the legislation explains, adding that any germline integration “creates risk of random human genomic modifications being passed on to the next generation of Americans.”
The measure blasts the lack of informed consent for recipients, pointing out that individuals are “not provided adequate information both as to the nature of the harm posed to them” and that they’re barred from seeking compensation under current federal law.
“Therefore,” the bill states, they “do not have the ability to give valid consent to have medical products employing this material or the delivery procedure administered.”
Significantly, lawmakers assert that the spike proteins in mRNA COVID shots may “be communicable to others (by a process known as ‘shedding’) and may cause side effects or harm even in individuals who are not the intended recipient.”
HB 4262 would strictly prohibit healthcare professionals from administering any “synthetic mRNA-based gene therapy product” within the state, unless used to treat noninfectious diseases such as cancer or rare genetic disorders.
It defines “synthetic mRNA-based gene therapy” as any product that introduces foreign genetic material into human cells to exert medical effects through transcription, translation, genomic integration, or genetic modification.
This includes:
Standard synthetic mRNA
Modified mRNA with pseudouridine
Self-amplifying mRNA (saRNA)
Any related biologic meant to prevent or mitigate communicable disease
Violating the proposed law would carry harsh penalties:
“Intentional or wilful violation… shall result in a suspension of the healthcare professional’s license… for no less than one year,” the bill states. Licensing boards could also apply additional penalties and fines at their discretion.
Licensing boards would be required to report any violations to the Director of the Department of Public Health, who must:
“Keep record of the violations for no less than seven years and… inform the General Assembly of the number and nature of violations no less than annually.”
The legislation was introduced and read for the first time in the South Carolina House on March 27 and was referred to the Committee on Medical, Military, Public and Municipal Affairs.
If passed and signed into law, the act would take effect immediately upon approval by the Governor.
With South Carolina now taking the lead, HB 4262 marks a bold legislative stand against what lawmakers call an “inadequately characterized potential public health threat”—and it could become the blueprint for other states ready to draw the line.
They are some sick people. You can change how your look, but you can’t change who you really are. You can change yourself into a green Martian, but you’ll still be mentally disturbed. Get well, not disfigured
A major peer-reviewed study of almost 100 million people has confirmed that Covid mRNA “vaccines” have caused a global surge in death and deadly disease.
The study documents the outcomes of 99 million people after they received Covid mRNA injections.
During the study, the researchers examined the official government data from eight countries.
Participants in the study included 99,068,901 Covid-vaccinated individuals.
The study has concluded that the injections are responsible for the global surge in sudden deaths and life-threatening illnesses.
The researchers found that staggering numbers of vaccinated people suffered serious complications such as heart failure, blood clots, strokes, brain disorders, and severely weakened immune systems.
Many of those tracked by the peer-reviewed study also died suddenly and unexpectedly.
The research was conducted by the Global Vaccine Data Network in New Zealand.
The study’s paper was published in the prestigious, world-renowned Vaccine journal.
Two decades ago, CBS aired a bombshell report on the flu shot, revealing a truth that health officials didn’t want to admit. Despite flu shot uptake among seniors skyrocketing from 15% to 65%, flu deaths continued to climb. It doesn’t fucking work and the whole thing is a farce.
NIH scientists were devastated. They expected the data to confirm the vaccine’s effectiveness. But instead, their own research shattered that assumption. So they assumed other factors must be “masking the true benefits of the shots.”
Sharyl Attkisson reported at the time, “No matter how they crunched the numbers, they got the same disappointing result. Flu shots have not reduced deaths among the elderly.”
Atkisson, the reporter in the above clip, later left mainstream news to become an independent journalist focused on exposing Big Pharma, government corruption, and mainstream media lies.
Going back to the story, the scientists looked at the flu shot data of other countries in hopes of finding more optimistic data. But what they found instead was “the same poor results in Australia, France, Canada, and the UK.”
A new search tool unveiled Friday increases public access to information about the connections between advisors to the Centers for Disease Control and Prevention on vaccine policy and the pharmaceutical industry.
The Advisory Committee on Immunization Practices (ACIP) discusses epidemiological studies, weighs the benefits and side effects reported in clinical trials, and makes recommendations to the CDC on the routine vaccination schedules for children and adults. The ACIP’s recommendations inform which shots are reimbursed by health plans. In a bid to enhance transparency around the process, the Department of Health and Human Services (HHS) has enabled users to search which advisors reported potential conflicts of interest and recused themselves from casting a vote affecting a drugmaker they had ties to.
The new tool is consistent with pledges by HHS Secretary Robert F. Kennedy Jr. to restore trust in the nation’s health agencies lost during the pandemic through increased information.
“In alignment with HHS Secretary Kennedy’s commitment to radical transparency, CDC released a tool for Americans to easily access conflicts of interest for ACIP committee members,” a CDC spokesman said in an email. “Rather than conflicts of interest being buried within meeting minutes, this tool quickly provides the public with ACIP members’ conflicts of interest.”
The ACIP became a flashpoint for controversy during the COVID-19 pandemic, reenergizing concerns about payments advisors receive from the pharmaceutical industry.









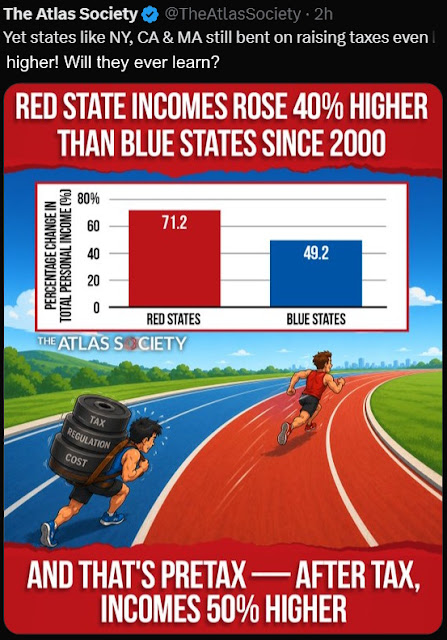
















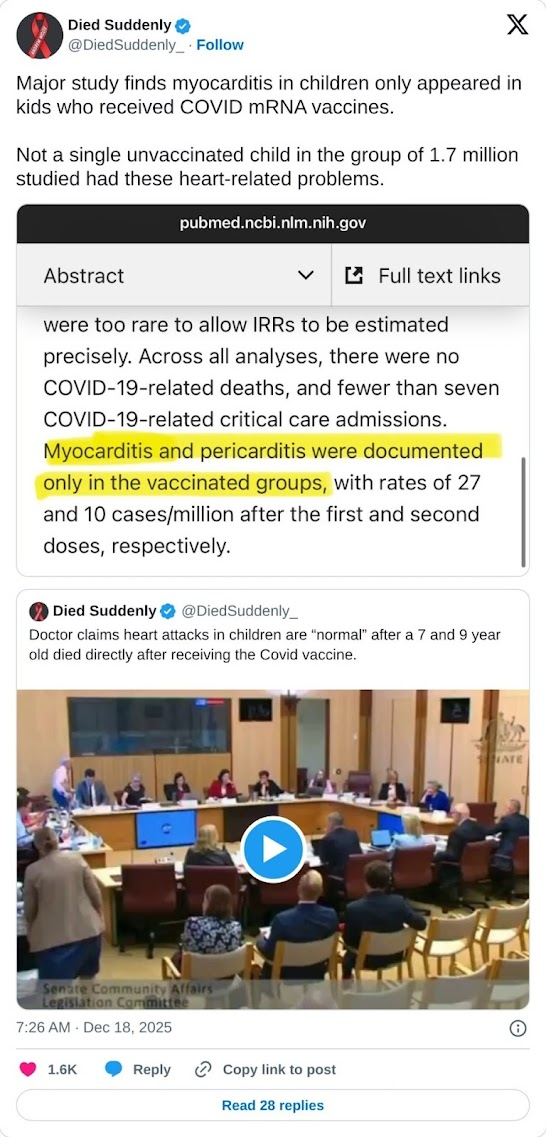



























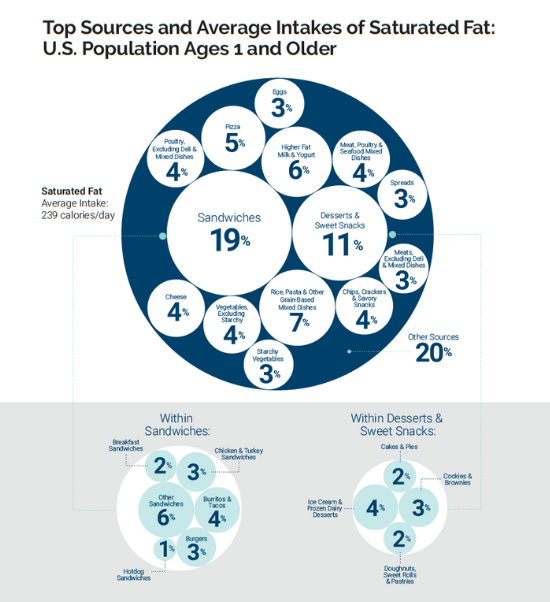

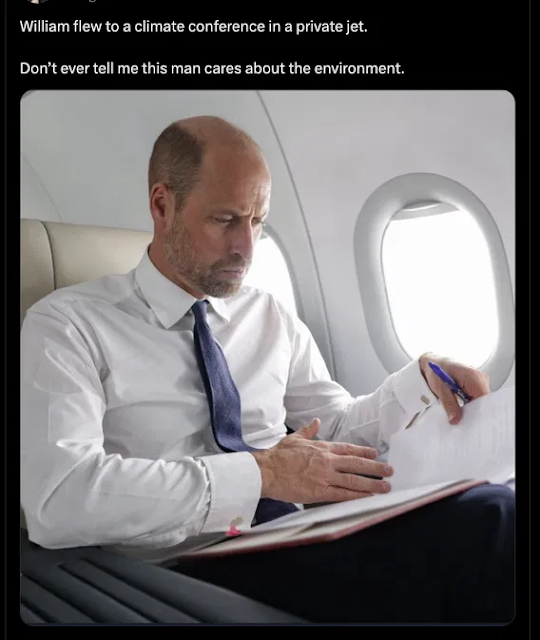





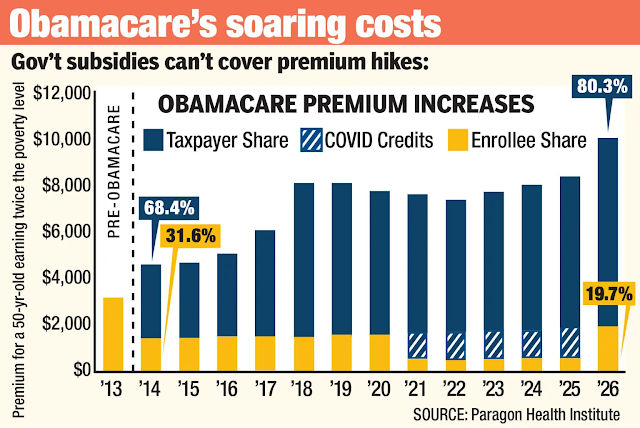


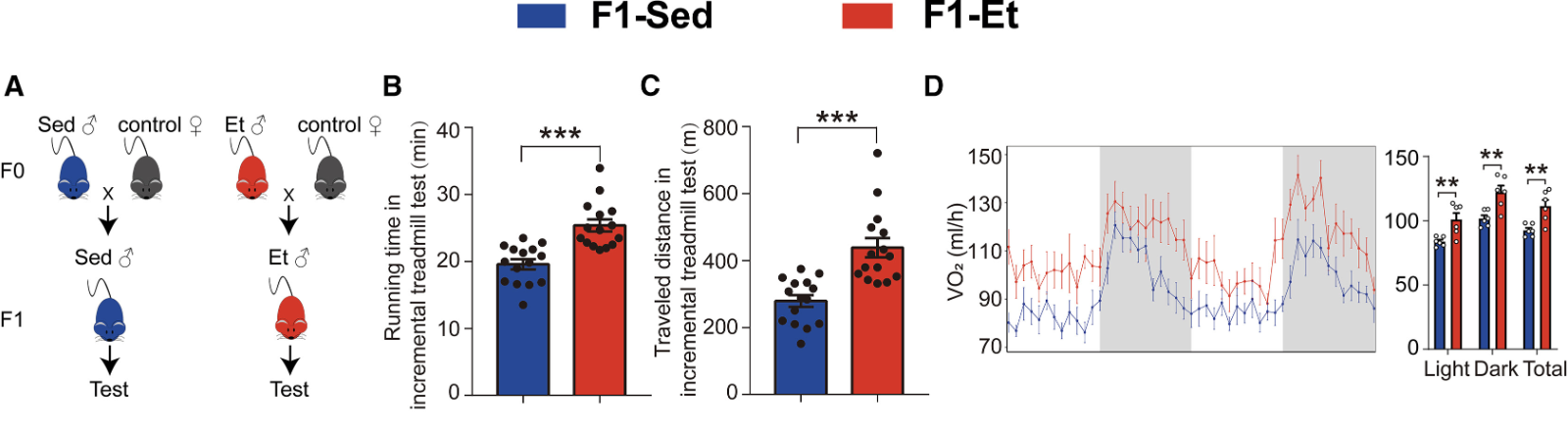
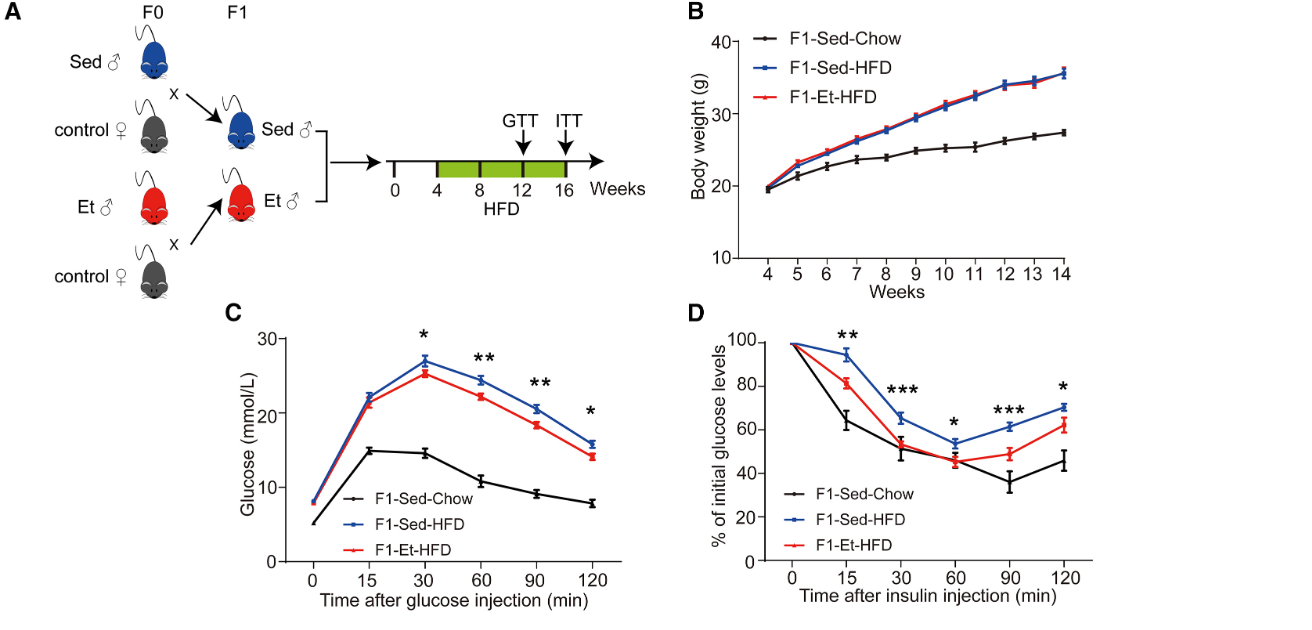
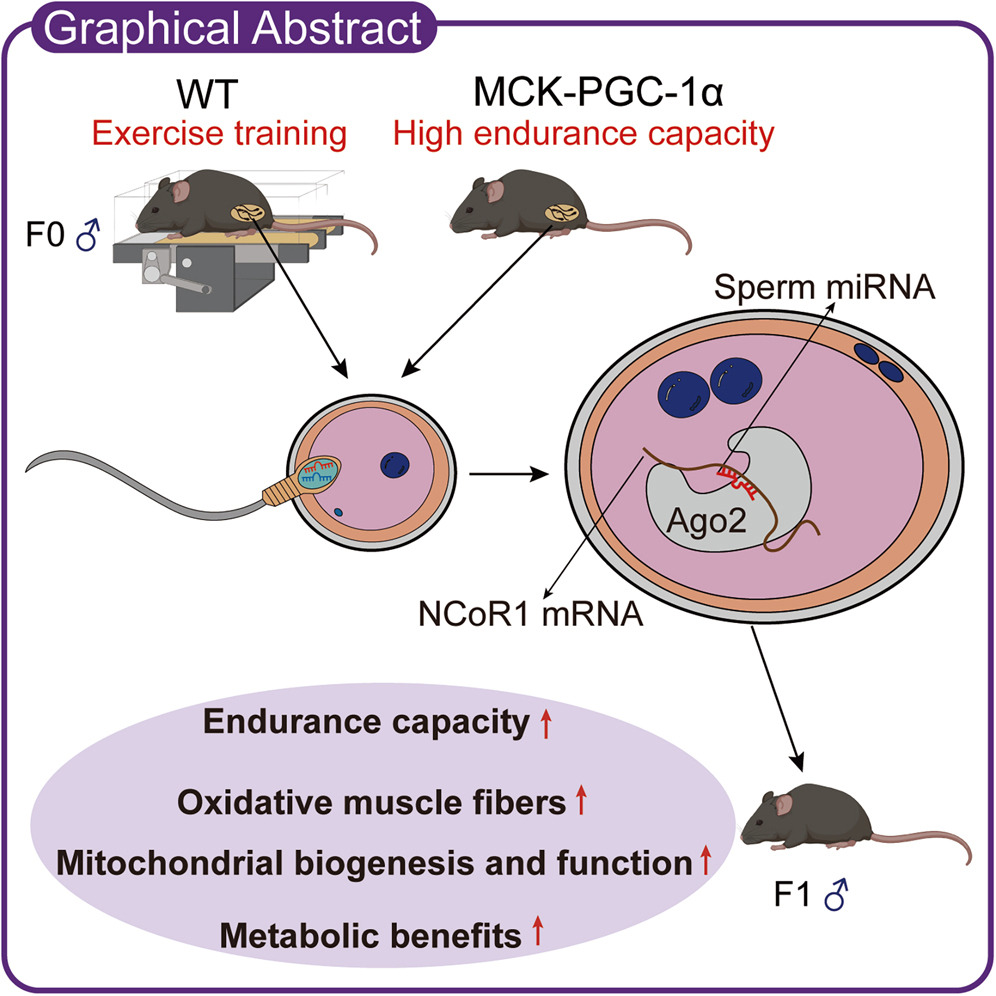







































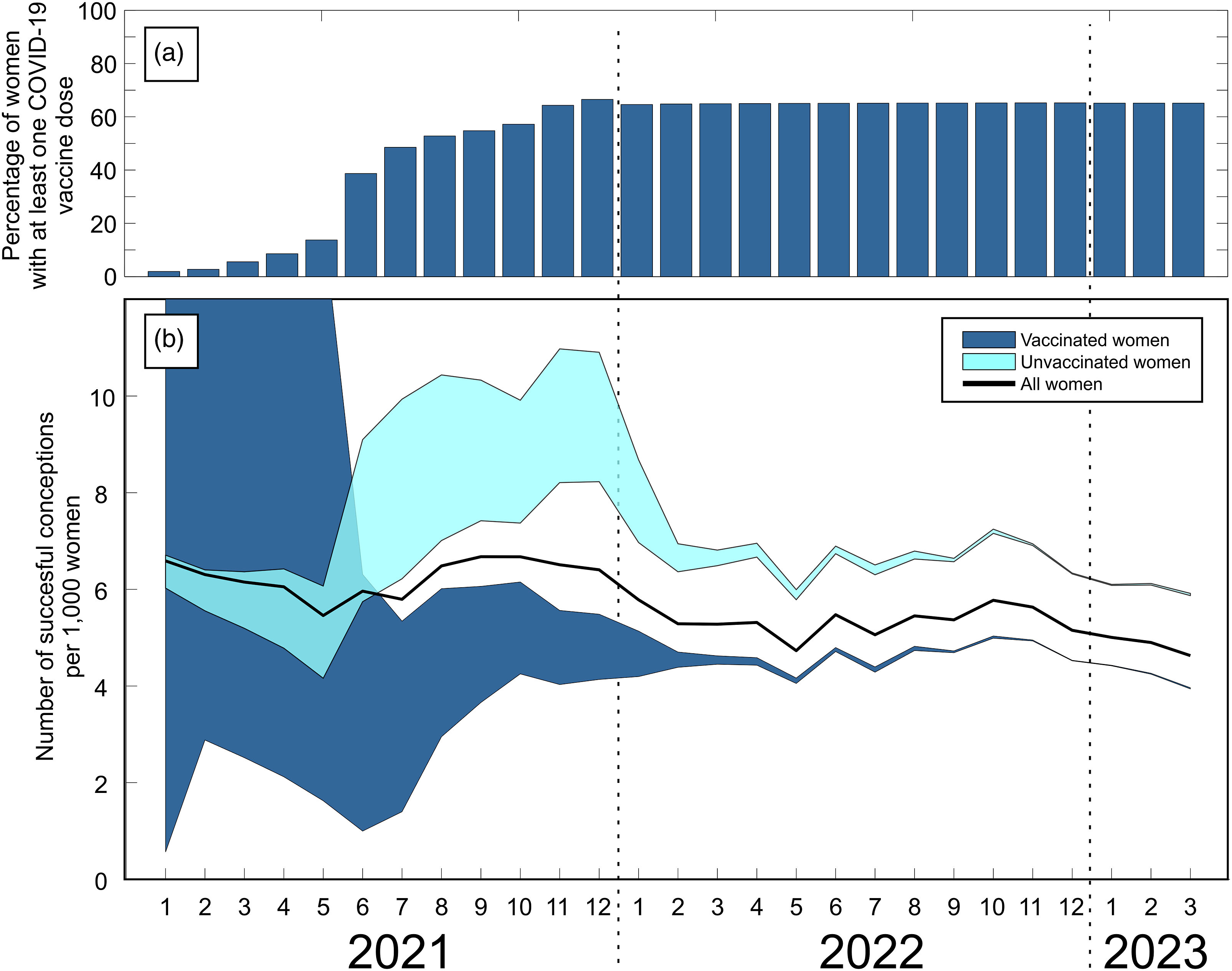



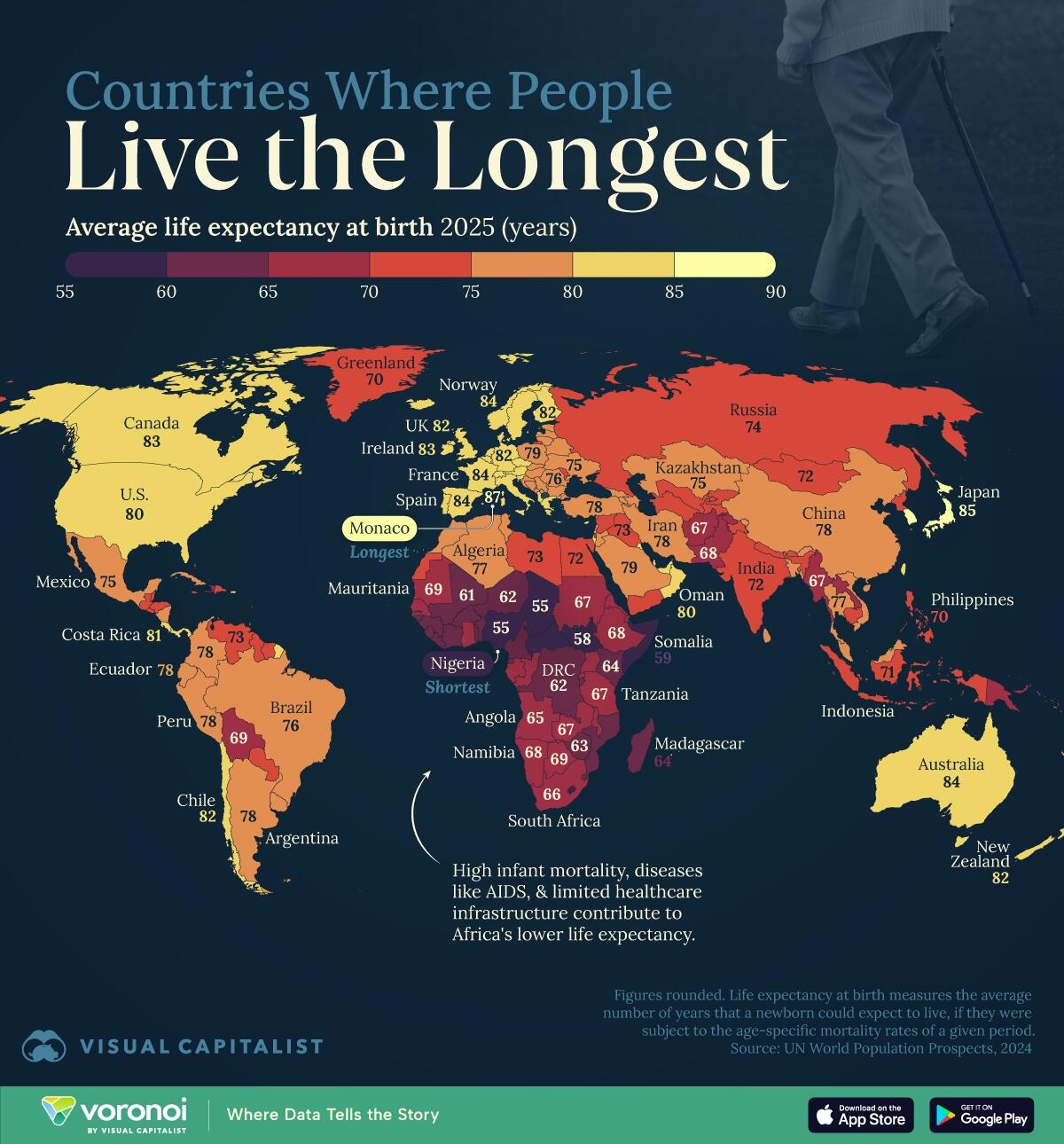




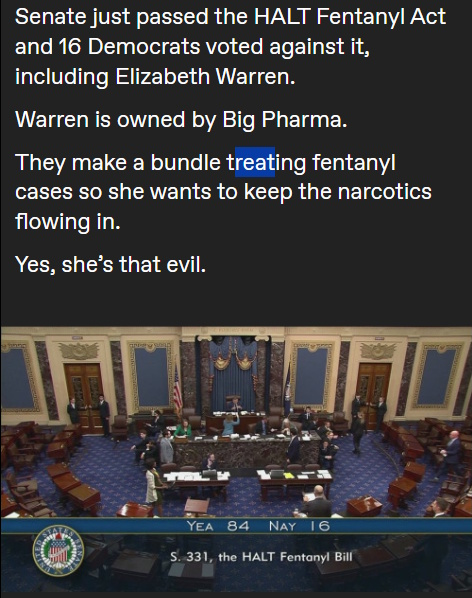


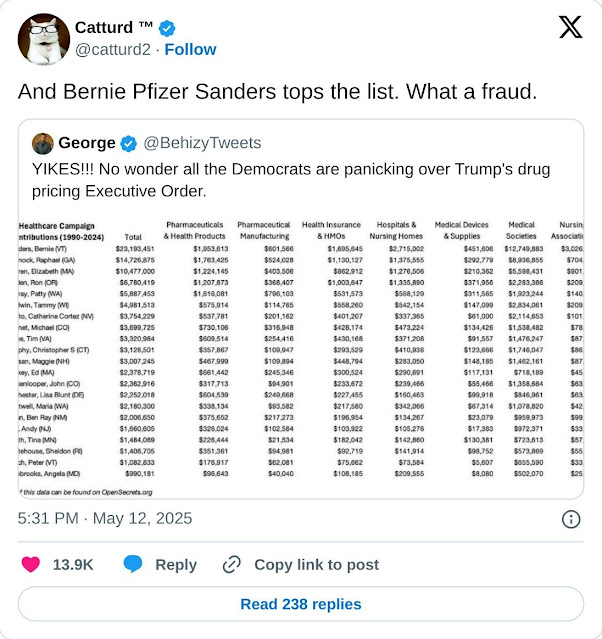





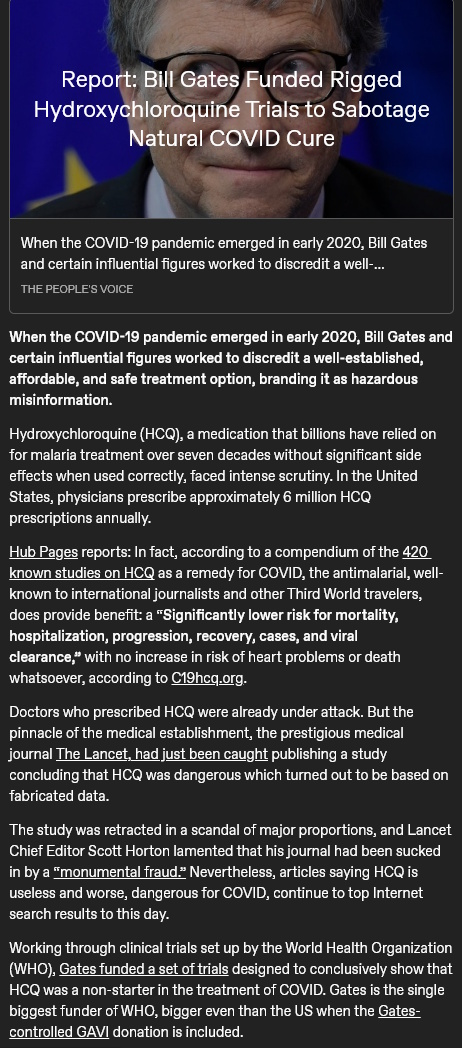

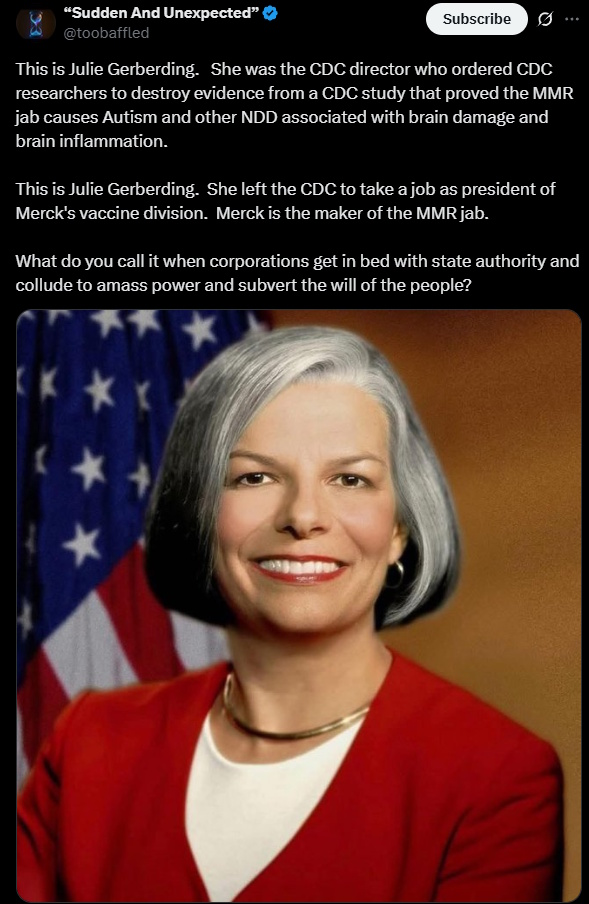


















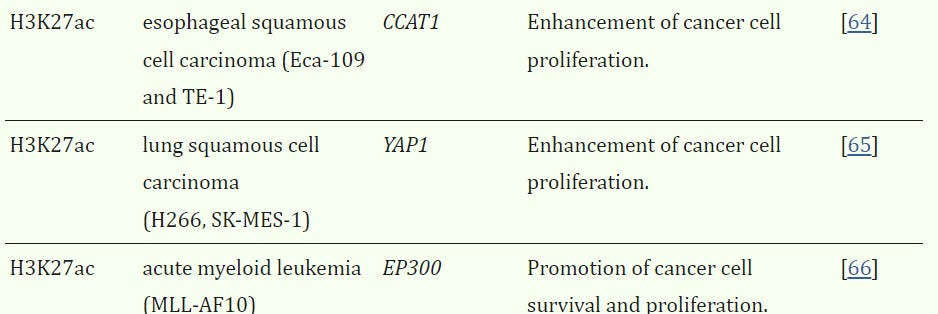

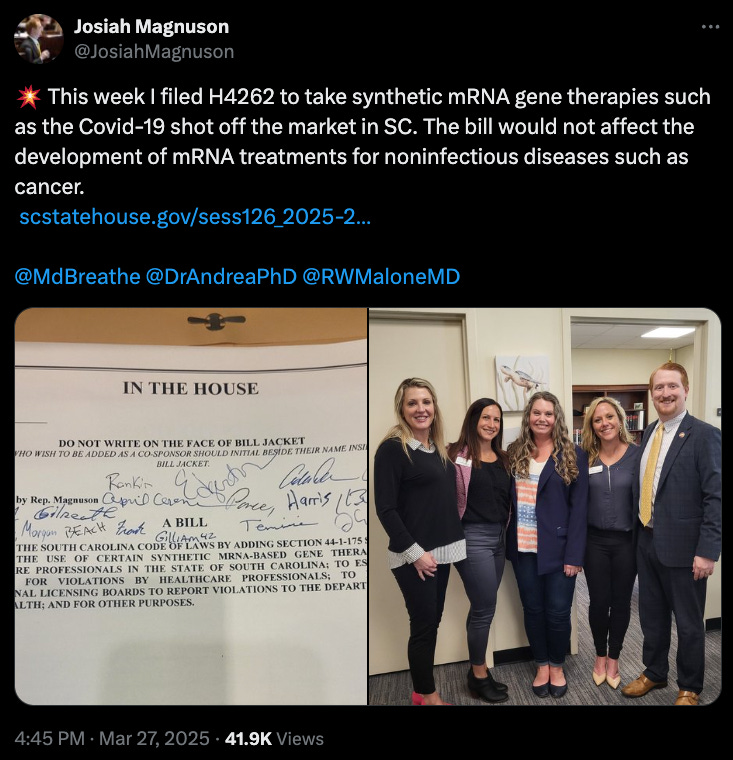
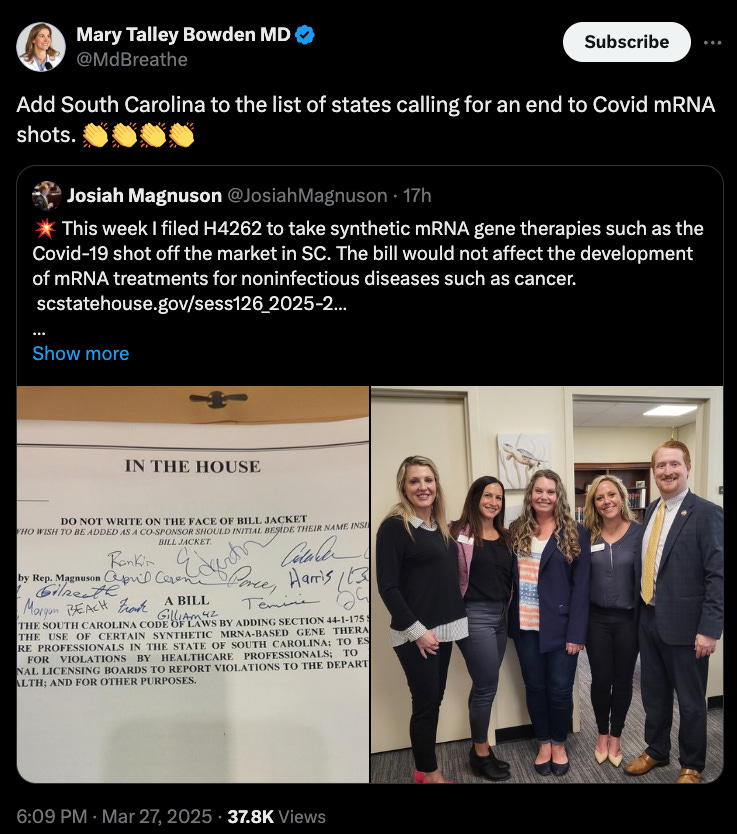




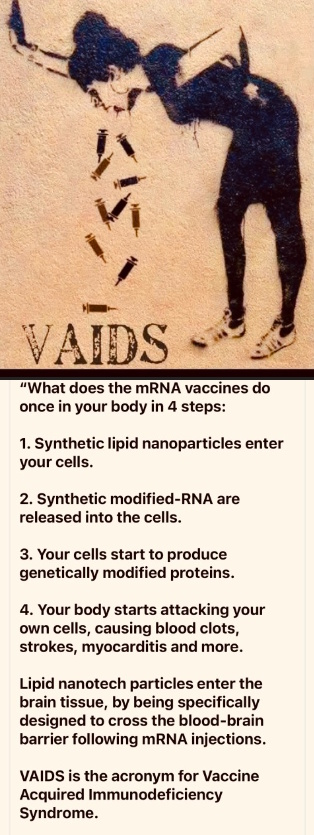

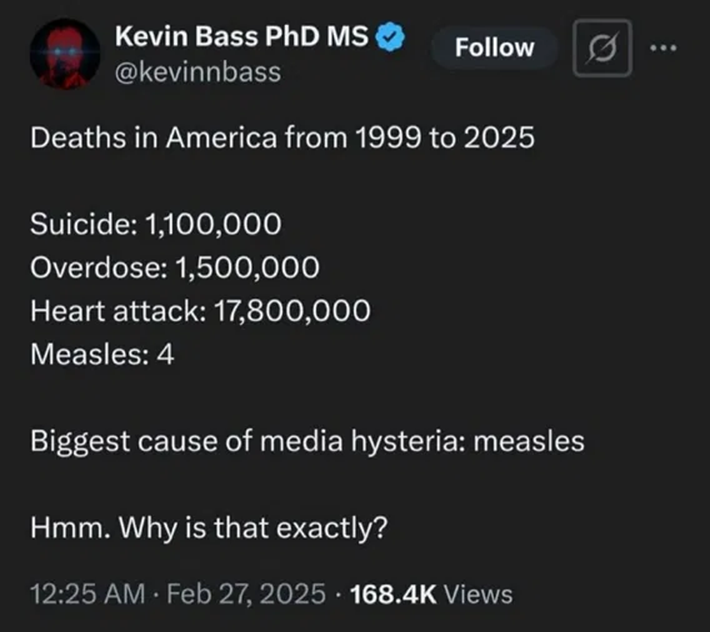
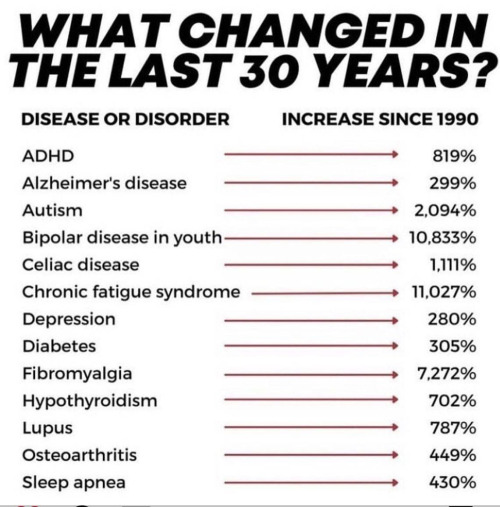
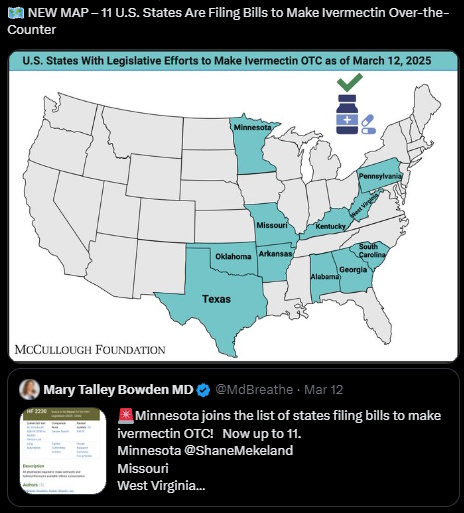








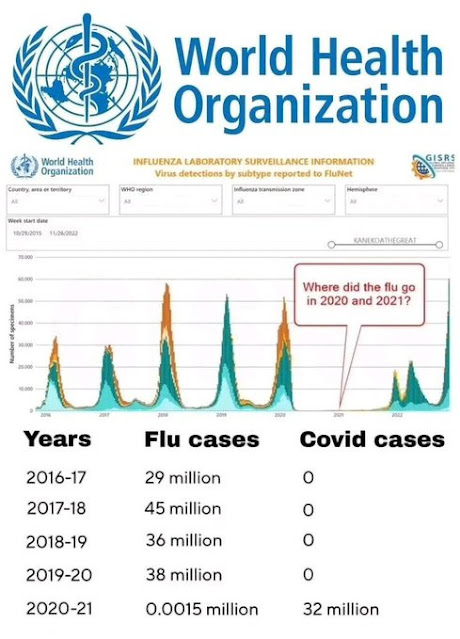



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}