
1
2
3
4
5
6
7
8
9
10
Cars
Every Inch of This AWD Porsche 930 Turbo Tribute Is Engineered to Be a Problem – only 11 made. Some of those owners will collect Darwing Awards
Health
5 Simple Pieces of LIFESAVING Medical Knowledge – hope I don’t have to do some of these
Tyrann Mathieu Almost Died From Drinking Bleach At LSU In Order To Pass A Drug Test – possible dumbass of the year. It proves you don’t have to be smart to play football.
Dumbass
Lottery Winner Hit With Lengthy Prison Sentence After Using Prize To Fund Massive Drug Ring – he could be a bigger dumbass than Tyrann above
EU
The EU Just Murdered Western Civilization – they no longer will be pure any country of origin. It will destroy sales of country specific products that we were used to associating with. It figures it was a female who would lead with her emotions rather than logic.
Anti-ICE or Anti-American
Philadelphia DA Sparks Outrage After Vowing to ‘Hunt’ ICE Agents Like ‘Nazis’ – what a dick. Why would you go against the law as a DA? Hopefully, karma will intervene
ICE Watch Is A Criminal Conspiracy – Shut It Down
Andrew Wilson Says Leftists Appeal Specifically to the Mentally Ill as a Tactic to Radicalize Them [VIDEO] – aren’t you mentally ill to be on the left anyway if you are older than 30? If you can’t figure it out by then, then you are like Tim Walz, a retard. They act like Nazi’s and experiment on the Unter-Menschen, the under people.
Obama – Deporter in Chief
Remembering “Deporter in Chief” Obama’s Most Lethal Border Blunder – why is it ok for Obama, but not Trump? Oh, TDS, that’s why
Celebtards
Left-Wing Celebs Escalate Attacks on Trump, ICE – this is why America hates actors. You pretend to be others for a living. Don’t pretend to be important or think that we care what you think. Just go away to your Hollywood parties that are out of touch with real Americans
FAFO
Fla. AG Uthmeier: Yanked Nurse’s License Over MAGA Post – It was a dick thing to say anyway. Keep politics out of your professional life unless you are a politician
What’s The Least Spoken Language In the World
Football
The NFL Is Getting Brutally Mocked for appointing a “Chief Kindness Officer” for the Super Bowl – Oh FFS, just Bud Light the league.
Virginia – FAFO
Virginia Voters Learning What FAFO Means as Newly Elected Democrats Lock and Load for Massive Taxes [VIDEO] – put a liberal white woman in charge and watch her destroy the state. You voters are dumbasses and did it to yourself.
Billionaire problems
What’s Worrying Billionaires the Most in 2026? – being that rich isn’t as great as it seems. You have problems other people don’t have to worry about. You can’t take it with you anyway. Have enough and the rest is meaningless
Longevity
Health in Every Bite: Top 10 Superfoods for Longevity and Disease Prevention
Disney
Sixth Dead Body Found at Disney World in Less Than Three Months
Health
A Core Cancer Therapy Is Being Ignored: Research Shows Fasting Exploits Cancer Cells’ Fatal Flaw
NIL Money
Who Are The Most Expensive Players In The College Football Transfer Portal By Position
Fantasy Football/Competitive Eating
Fantasy Football Punishment Nightmare: Bro Must Eat Hot Dogs For Every Meal Until He Matches Joey Chestnut’s Record – 71 is a lot of dogs
FAFO
Hilton Drops Minneapolis Hotel That Lied About Immigration Agent Ban
NASCAR Commissioner Resigns Over Texts Revealed in Michael Jordan Antitrust Trial
Russia
Retired Russian Col. Gen.: Everything in Russia Is In Bad Shape – like before the fall of the USSR
For The No Kings Crowd
ICYMI: GOP Sen Claims Biden FBI Placed ‘Innocent Americans’ Under Surveillance, Including Catholic Teacher – They actually did what they accused Trump of maybe doing
Vacation Shitholes
The 39 Countries Where You Can’t Vacation in 2026 – They have one obvious thing in common and being a shithole is not it. People are trying escape from these places, not go to visit.
Feminists
Campus Sexual Violence Rate Closer to 1%, Not 25%, Study Suggests – it doesn’t fit their all men bad narrative though. Once again, liberal women are one of our biggest problems
Cars
A Real Petty Blue 1972 Plymouth Road Runner Survivor Just Hit the Market
2027 Dodge Charger Hellcat V-8 Is a Return to Form Worth Waiting For
The Theft of Taxpayer money and misuse by Government
Three Examples of the “Theft Industrial Complex” in 2025 – with stuff like this happening, we’ll never balance the budget or stay a great nation
Sports
The 13 Richest Athletic Departments In College Sports Valued At More Than $1 Billion
The 12 Most Impactful Transfers In College Football History
Avengers Doomsday
Professor X, Magneto And Cyclops Return In Epic, World-Ending Teaser For ‘Avengers: Doomsday’ – so the woke movies failed and now they are bringing back the real heros’s. The real Captain America (Steve Rogers), Thor and a bunch of other white guys who made billions because the movies were good.
Energy and the Climate Hoax
Analysis: Don’t blame AI’s data centers for rising rates: ‘Electricity prices are rising fastest in states pursuing green energy policies, including California, Massachusetts, & New York’ – so much for the Green New Deal. It’s the same thing for prices in the EU for countries that fell for the Climate Hoax
U.S. Seizes Venezuela-Linked Oil Tanker in North Atlantic – Got it. less for Hezbollah, the bad guys
California
California Faces Fuel Disaster As Refineries And Gas Stations Shut Down – they can use their EV’s to get around. They don’t need gas and they hate it anyway. Now try and live without it. IT’s not just Tim Walz that is a retard, try Gaven Newsome
Healthcare
Unleashed: Retired Nurse Can Finally Speak Out About Flu Shots and Doesn’t Hold Back [VIDEO] – it’s a hoax like the Covid jab and doesn’t work. She explains how she never took the shot, health with 300 patients a day who had it and never caught the flu
Yes, processed food is full of sugar. But hold on, this clip will actually blow your mind…
Drinks to impress a bartender
FBI
FBI Ignored Epstein Child Porn Warning for Nearly 10 Years – sick people
Election Interference
Ex-FBI agent says Bondi has ‘slam dunk’ conspiracy case against Obama’s feds for election meddling…– and she’ll do nothing about it, like the whole first year
Wind Farms
Wind turbine eagle-kill secrecy may soon end – good, I’m for protecting nature. Wind power can’t pay for itself anyway. Scrap the whole thing. They also deicmate bats and other wildlife
Government Mismanagement
German Govt Signals “Challenging Years” Of Austerity Ahead While Spending Billions On Ukraine & Immigration – Stop letting in the illegals and fuck the Ukraine. They have Putin as the next Stalin, but they have much bigger problems at home, like all the goat humpers they let in.
Trust
Where People Trust Each Other Most (And Least) In The World – factor in Islam and it makes a lot of sense
Cars
This one is going to go for a lot of money like the other one.
BLM
BLM Birmingham, Alabama Co-Founder Who Accused Cops of ‘Racism’ and ‘Violence’ Gets Busted on Domestic Violence Charges – Whines About Conditions in Jail (VIDEO) – and continues to be the farce that it’s been, helping no one but themselves, not any black people.
Air Travel
Man Charged After Allegedly Trying to Open Plane Door Mid-Flight, Yelling ‘We’re All Going to Die’ – just another reason I hate to fly
Politics
Report confirms there was a ‘Russia, Russia, Russia,’ only it involved DEMOCRATS – Forking iceholes
Crime and Disgusting
For the Love of Everything Decent, Put Some Clothes on if You’re Going to Steal a Patrol Vehicle
Cheaters Who Work For ESPN
Football
James Madison Has An Expensive Secret Weapon Fueling Its College Football Playoff Run – pay to play
The 17 Players Who Won The Heisman Trophy And A National Championship In The Same Season
10 Of The Greatest Individual Bowl Game Performances In College Football History
Best Men’s Faces
Dr. Douglas S. Steinbrech, Leading Male Aesthetic Surgeon, Reveals Top 10 Most Requested Male Faces of 2025 – I knew it wasn’t me
DNA
DARPA Is Working on Synthesizing DNA With Light and the Luciferian Parallels Cannot Be Ignored – they were in on Covid and the Jab also. They also invented the internet. None of that is very good
Health
New Study Reveals Prediabetes Remission Cuts Heart Disease Risk by Over 50%
Economy
Lower Gas Prices to Save Drivers $500M Christmas Week – NBADJT
War On White Men
Apple kicked off the WAR on white men… – and we will pay for this. The world needs men.
The Media Backs up the Anti-White Wing of the Democrat Party
Islam
All of France is a No Go Zone Now – France is fucked. Islam has taken the French out of France
Food supply
Cars
Ford Retreats From EVs After Billions in Losses – nobody wants them either
The First V-Code Cuda Convertible Produced, Serial No. 4 – it’s rare, but I bet the hemi-cuda’s go for more
EU Backing Down Off 2035 ICE Vehicle Ban – Because the EU is retarded to believe in it in the first place. Get back to reality.
Crime AT BARS
Rare Earth Minerals
Utah’s Desert Yields Rare Earths Motherlode, Challenging China’s Grip on Critical Minerals
Masculinity
Erasing Masculinity Has Created a Generation in Crisis – Men have saved the world time an again. It’s why the feminists want to try and erase it. We have to stop these PC SJW.
Your gut microbiome is filled with trillions of microorganisms and microbes that are integral to your overall well-being. The gut microbiome is home to both good and bad bacteria, which both play an essential role in our overall health.
The food we eat plays an important role in shaping this microbial landscape. Certain foods can nourish our good gut bacteria, supporting diversity and balance. In contrast, others can wreak havoc by empowering the harmful bacteria, causing an imbalance that can lead to poor gut health. Understanding which foods to embrace and which to avoid can provide a roadmap to a healthy gut.
Here at Gaia Herbs, we believe in nature’s healing and restorative powers. Let’s cover the importance of gut health, the best and worst foods, and a few of our supplements that can help. Let Gaia Herbs be your guide on the journey to a balanced and healthy gut microbiota.
When you think of the gut, you probably think of digestion. But the truth is, the role of our gut health extends far beyond breaking down the food we eat. It’s a complex system intricately connected to almost every aspect of our health.
Let’s get a little deeper into the multifaceted roles the gut plays in our body:
More here it’s interesting
Incest
Muslim Country First Cousin Marriage Rates and Average IQ Statistics Are Shocking [VIDEO] – producing idiots, or robots that won’t grow out of the 7th century and will kill willingly
Cars
Revived V8 Chevrolet Chevelle Is the Full-Size Five-Seat Virtual Answer to the New Charger – It used to be a bad ass car. Good old horsepower instead of the Electric Car nonsense. It sounds so much better.
VW Aims To Cut Development Costs In Half With New “Made In China” Car – what does this say about the German Economy? Also, I’d rather have German engineers than Chinese
Healthcare
EXPOSED: US Labs Breeding Deadly Foreign Ticks in Bid for mRNA Vaccines – those bastards are trying to kill us
Tariff’s And Economy
BLOOMBERG: Trump Was Right On Tariffs, All The Really Smart Economists Were Wrong
Climate Hoax
Gross And Disgusting
The 5 Worst Restaurant Franchises
Education
DEI Policies Are Making American Students Dumber
Public Perception of Higher Education is Shifting Negatively
Flu
Pfizer’s mRNA flu shot failed its pivotal clinical trial in adults 65 and older… – of course it failed.
Political Strategy
Five Minutes of Homework Would Spare Dems Days of Grief – How and why Democrat strategy has gone wrong
Money
U.S. Treasury to Seize Remittances Sent Abroad by Illegal Migrants — Transfers Over $2,000 Will Be Flagged as Suspicious – no more sneaking money out of the country, it’s been going on too long.
Tariffs
Tariff Revenue Hits Record $31 Billion in October — As Trump Floats Abolishing Income Tax Altogther! – NBADJT
Death
Japanese legislator refuses to allow Islamic cemetery for reasons both cultural and scientific – a different reason than you’d expect, but the goat herders still won’t like it
Treason
BlackRock’s Larry Fink Is as Dangerous as You Thought
Indisputable Fact: Biden’s Policies Brought Terrorists Into America – except it was also a group of handlers who told him what to do
Idiots in Congress
Klobuchar Face Plants the Trump Inflation Narrative
Covid Vaccine
FDA Admits COVID Vaccines Led to Child Fatalities…
Animals
Massive Moose Caught on Camera in Very Unexpected Location, Photos Are Majestic
California Man Captures Footage Of Massive Bear That’s Been Living In A Crawl Space Under His House
Bigfoot
Declassified Documents Reveal FBI Correspondence With Bigfoot Organization – Well, he’s the champion of hide and seek.
Christmas
Portland Refuses to Call It a Christmas Tree – a bunch of heathens who live in a shithole. Enjoy hell when you get there.
Nature
USA
America’s Real Enemy – and it will be hard to defeat
‘Oh, F*ck Off!’ Democrats Rage at ‘Pathetic’ Shutdown ‘Betrayal’ in Mass Backlash
“At What Point Does This Become Treason?”
Artificial Intelligence
How AI Is Supercharging Scientific Fraud
DOGE
DOGE: U.S. Government Agencies Terminate 67 Wasteful Contracts Worth $1.4 Billion
Communism
White House Declares ‘Anti-Communism Week’ Honoring 100 Million Lives Lost
Islam
‘I Beat Hitler’ – Survived Dauchau only to see the election in NYC
Cop30
UN’s Clear-Cut30: Morano on Real America’s Voice TV: ‘Brazil has clear-cut up to 8 miles of virgin tropical, Amazon rain forest at this summit…in order to bring in the private jets and the limousine’ – Hypocrisy, thy name is Climate change. Let’s not forget it started out as AGW. Antrhropogenic Global Warming. Humans didn’t do anything other than scam others for money. It was the same formula BLM used.
Government Shutdown
Speaker Johnson calls House back to end shutdown as Jeffries urges Democrats to oppose deal – because it cuts off the money laundering through the insurance companies back to the dems. They don’t care about insuring the people. It ends their control and push to socialized medicine.
Snow Skiing
Watch: The Greatest Ski Descent in History… Everest’s Stunning Hornbein Couloir… – There’s a dragon I don’t have to slay
Jobs
China’s DeepSeek Issues Rare Warning Of An Incoming AI-Fueled Jobpocalypse – it pays to be a carpenter or a plumber. office and administrative jobs are going to get the sword
Lying
Eric Swalwell Names Washington DC Home as ‘Principal Residence’ and Has No California Address – combine that with sleeping with Fang Fang, the Chinese spy and you have a real loser here.
Quantum Computing
Quantum Computers Model Complexity of Materials – It will challenge the limits of current computing and surpass it.
UK
‘A wicked wife’: The truth about Tudor England’s ‘most hated woman‘ – by the time I read it, I hated her also.
EV’s
Mercedes Slashes Prices by Up to $50,000 as EV Inventory Piles Up – Nobody wants them. Even Porsche is cutting back. The Ford F150 Lightning is dead also
Seal Team
SEAL Team 6 Operator Reveals High IQ Move To Kill Osama Bin Laden: WATCH – I never get tired of this story
Health
Study Finds That Common Dry Cleaning Chemical Tetrachloroethylene Linked to Severe and Potentially Fatal Liver Damage – all of those clean clothes killing people
China Spying
‘Wreak havoc’: U.S. nuclear bomber fleet shares fence with trailer park linked to Chinese intel-tied fraudster – No, they aren’t spying, they’re just running a trailer park
Islam Practices
Muslim Preacher Says Americans Are So Uncivilized and Backward That They Use Toilet Paper – back to 600 AD we go by starting in NYC and Minnesota. Stop it now so we don’t have to have a Gates of Vienna.
Obamacare
The Obamacare Secret at the Heart of the Shutdown: Insurers Made Billions at Taxpayer Expense – Lies, lies, lies from the start. It was always about the money and socialism, not healthcare.
Doctor Lays It Out So Clearly: Barry’s Affordable Care Act Was the Biggest Shakedown In US History…
Illegals
If You Move the Third World to the First World, Eventually We Become the Third World – Look at the UK, Rapes in Sweden, Germany Economy. Stop it at NYC now before it ruins the US.
Quantum Computing
Space: The Final Frontier – A financial opportunity for a technology searching for money.
Quantinuum Makes Another Milestone On Commercial Quantum Roadmap – Who has the advantage?
Media (and Lying, but then I repeat myself)
Trump may squeeze the boobs at the Beeb – Anti-Americanism at its’ best
Another How Woke and Feminism is ruining everything they touch.
Born Perfect: The Girlboss and the Death of Growth… – From ruining Star Wars to businesses. Why Luke Skywalker had to suffer to become a hero. Men had to learn to lead the hard way and this shows why the lessons have to be learned. You can’t just DEI your way to be a leader. 2 of my 3 worst managers were girls. They made life this difficult.
Double Standard for the Elite
“Clinton Corruption Files” – Bondi, Patel Give Congress New Evidence Detailing Clinton Foundation Corruption – They clearly not only broke the law, but mocked others. They’ll also get away with it. It’s like they have evidence on others that is blackmail.
Academia
The Dirty Secret Behind America’s “Best and Brightest”: The Foreign Cheating Scandal Academia Won’t Touch – Cheating in Ivy League schools, I’m shocked
Illegals
‘If you move the third world to the first world, eventually we become the third world’ – Look at Germany, Sweden and the UK.
Cars
One of 48 Original Ford GT40 Mk1 going to Auction at Mecum in Spring.

TV
Disney/ESPN Losing $30 Million/Week Amid YouTube TV Blackout, According To Industry Expert – And I’m missing Jeopardy and Football. At least I can see F1 on F1TV because the BBC coverage is on ESPN, and it sucks.
Sports
The 5 Times A College Basketball National Title Was Won On A Buzzer Beater Or Last-Second Shot
Scientists at St. Jude Children’s Research Hospital explored how mutations in mitochondrial DNA contribute to cancer, the extent of their impact, and when and how they become a factor.
Mitochondria act as energy factories in cells and have their own, separate DNA. Mutations to mitochondrial DNA (mtDNA) have been observed in cancer, but it has been unclear how these changes might affect cancer growth. To find answers, St. Jude Children’s Research Hospital scientists combined computational tools and DNA sequencing technologies to examine these mtDNA mutations in cancer cells closely. Their new method lets scientists pinpoint when these mutations occur, how they change as cancer develops and whether they affect how cancer cells behave. The results of this study were published today in Science Advances.
Exploring the role that individual mtDNA mutations have on cancer has historically been difficult. “Each cell contains hundreds of copies of mitochondrial DNA; so, a mutation might be present at low levels in many cells, or at high levels in just a subset of cells,” said corresponding author Mondira Kundu, MD, PhD, St. Jude Department of Cell & Molecular Biology. “These different patterns can have dramatically different effects on how cells function.”
To overcome this challenge, the team combined several techniques, including powerful computational tools, statistical analyses, bulk whole genome sequencing and single-cell studies. This approach allowed them to determine how much mitochondrial DNA was mutated in each cell, and when these changes happened in relation to cancer development. Surprisingly, the researchers found that some mitochondrial DNA mutations occur before a cell turns cancerous — and that these mutations are not always random. It appears that in some cases, cancer cells actively “select” for a mix of normal and mutated mitochondrial DNA.
“This approach allowed us to tell apart harmless ‘passenger’ mutations from those that may help cancer grow,” Kundu explained. “That’s something the field has struggled with until now.”
Kundu’s team took the analysis further by deploying a tool, called NetBID2, created by co-author Jiyang Yu, PhD, St. Jude Department of Computational Biology interim chair. With this tool, the researchers found evidence that mtDNA may contribute to therapy resistance. They discovered a mtDNA mutation linked to changes in pathways associated with resistance to glucocorticoids, a common therapy for acute lymphoblastic leukemia. Further analysis suggested that this type of mitochondrial mutation may make leukemia cells more likely to resist treatment.
While this research highlights the role mitochondrial DNA mutations might play in leukemia, the main achievement is the creation of a novel multidimensional approach to investigate mtDNA. Kundu is optimistic about the value of digging deeper into this overlooked feature of cancer growth.
“This work shows that mitochondrial DNA can influence both how leukemia starts and how it progresses,” said Kundu. “The next important step is to apply this approach to many more patient samples, so we can fully understand its impact.”
Anal pain, really? I use AI quite a bit. I find that while ChatGPT is probably the most popular, I get the worst results, other than for coding. Even then, I don’t trust it. There are many options available, so choose your own. I use multiple, but stay away from this one
Here’s your butt story:
Consulting AI for medical advice can quite literally be a pain in the butt, as one millennial learned the hard way.
The unidentified man tried to crudely strangle a gruesome growth on his anus, becoming one of several victims of AI-powered health guidance gone terribly wrong in the process.
Many documented cases confirm that generative AI has provided harmful, incomplete or inaccurate health advice since becoming widely available in 2022.
“A lot of patients will come in, and they will challenge their [doctor] with some output that they have, a prompt that they gave to, let’s say, ChatGPT,” Dr. Darren Lebl, research service chief of spine surgery for the Hospital for Special Surgery in New York, told The Post.
“The problem is that what they’re getting out of those AI programs is not necessarily a real, scientific recommendation with an actual publication behind it,” added Lebl, who has studied AI usage in medical diagnosis and treatment. “About a quarter of them were … made up.”
By Dr. Philip Ovaida
As a heart surgeon, one of my favorite mantras is “hit your protein goal.” That’s because many of the patients who walk into my office see enormous metabolic improvements just by swapping dietary carbs for protein.
But maybe you’ve seen research talking about the unhealthiness of high-protein diets. Will getting rid of carbs increase your risk of a heart attack? Or will the amino acids in meat trigger cardiovascular disease?
From a purely scientific standpoint, probably not.
But I’ll go through the research so you can decide for yourself.
Let’s start with the studies sounding the alarm about getting ‘too much’ protein in your diet.
One posited that eating more than 22% of your calories from protein could raise cardiovascular and metabolic health risks.
Another found that “high-protein diets increase cardiovascular risk by activating macrophage mTOR to suppress mitophagy.” In other words, that high protein intake could overstimulate certain immune cells, leading to artery damage and higher cardiovascular risk.
Here’s a quick breakdown of their hypotheses:
So researchers concluded eating more than 0.8 grams of protein per kilogram of body weight could be harmful to your heart.
Now, before you start wondering if going vegan is your only option, I’d like to point out a few limitations.
For all these reasons, among many others, we lack concrete data to say high-protein diets are “bad” for the heart. High protein may actually be critical to those recovering from heart attacks or reclaiming metabolic health.
One study found that high-protein diets improve weight loss, reduce triglycerides, and improve HDL cholesterol, all of which are protective for the heart.
We also also know people lose muscle mass and bone density due to inactivity and inflammation after a heart attack. A higher protein intake can help maintain this lean body mass, which supports exercise tolerance and recovery moving forward.
This complements yet another study: higher protein intake after a heart attack may improve long-term patient prognosis. According to their analysis, heart attack patients eating high-quality protein had a much lower 10-year cardiovascular risk score compared to patients eating +50% less protein per week.
First, nutrition science is still quite young. It’s been less than 100 years since we isolated the first vitamin, after all. The science isn’t settled, and there’s still much to learn, so it shouldn’t come as a surprise that we’re still exploring new biomechanisms.
We also have to look at differences in terms and study structure. There’s a big difference between studying metabolically unwell young people versus metabolically healthy older adults, for example.
And don’t forget that N = 1. One person’s response to protein won’t be the same as someone else’s, especially within unique age, sex, or health cohorts.
But I can confidently say that the benefits of protein far outweigh any warning to the contrary, especially for those recovering from poor metabolic health.
Protein has become quite the target for misinformation. If you’re active on X, you likely know what I mean.
I can’t dispel all protein myths here, but I felt it was appropriate to cover a few topics.
First: most people actually underconsume protein, not overconsume it. Americans have a mean protein intake of 16%, which is less than half the max range of even US food pyramid RDVs.
And no, high protein isn’t bad for the kidneys. If you live with liver and kidney problems, then yes, you may need to plan your meals. But this applies only to a very small portion of the population.
When healthy, resistance-trained adults consume high-protein diets (think 3x higher than recommended daily values), there is no evidence of harmful side effects on kidneys and renal function. You can find details of that in this study and this one.
So please: don’t believe for one second that increasing your protein intake will do more harm than good. If you’re looking to repair, restore, or protect your metabolic health, a high-protein diet will be an incredibly powerful tool.
No, not at all. Especially not as part of a metabolically healthy lifestyle.
And if you’re at high metabolic risk, it might be worthwhile to increase your macros.
That means:
High-protein diets aren’t a danger to your heart health. For the vast majority of people, it’s one of the best lifestyle changes you could make.
If you’re not sure how to get started, I’ve written quite a few guides. Learn more about using high-protein diets to support your heart health in the following resources:

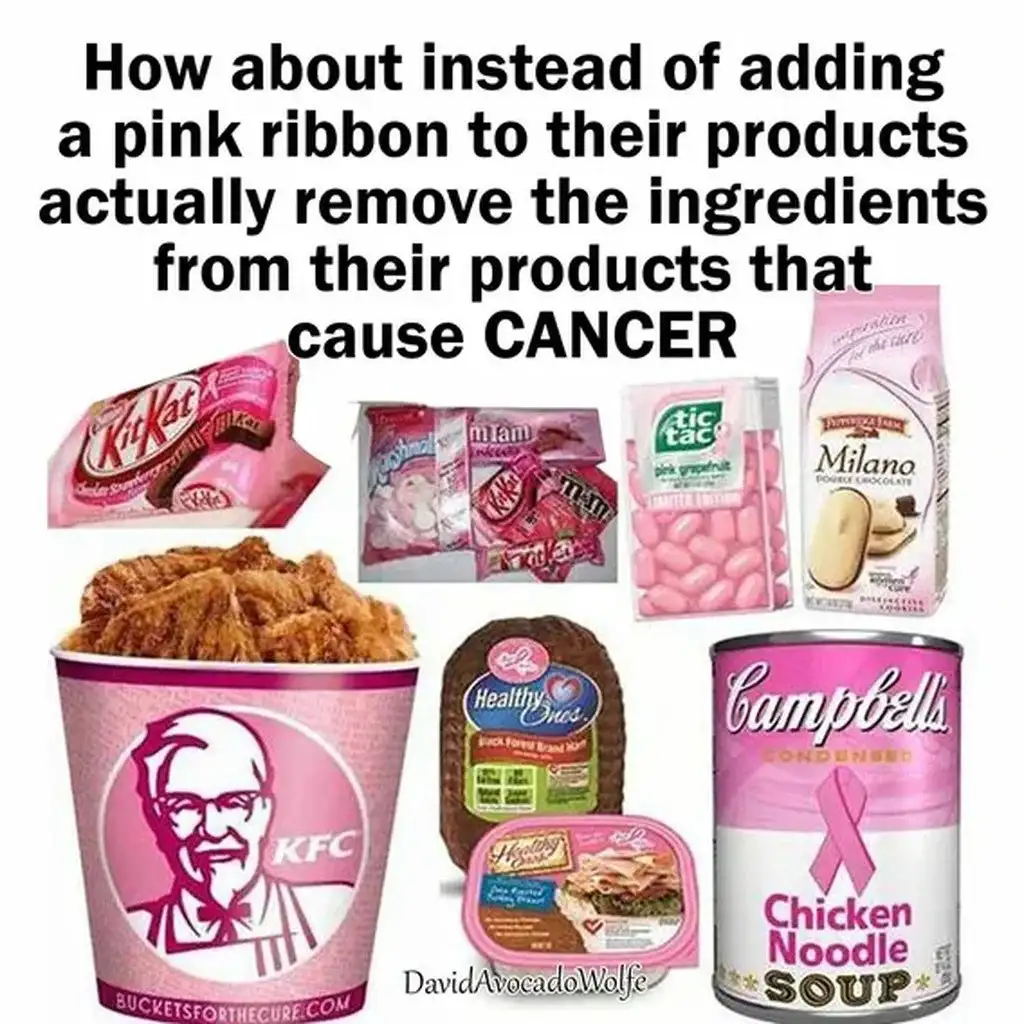
I lost my Mom to breast cancer. She beat it twice and battled it for 3 decades. In what amounts to malpractice, she ultimately succumbed to it. I do not take it lightly. So before you get outraged and be a SJW Karen with your panties in a wad, read the following and see what should happen if you do more than wear a pink ribbon. There’s a ribbon for every cause, but taking action to cure it is the ultimate expression of support.
Original article and source start here.
Once again, it’s “Breast Cancer Awareness Month,” as we’re hit with pink ribbons and fundraising alerts from breast cancer groups.
Two organizations that solicit funds purportedly for fighting breast cancer are the Susan G. Komen Foundation and the Breast Cancer Research Foundation (BCRF).
Wouldn’t you assume that groups promoting breast cancer awareness want women to actually decrease the risk by having women know all the risk factors?
Yet the biggest promoters of Breast Cancer Awareness month either omit the abortion factor or actually deny it.
Typically, these groups list lower risk factors that line up with their pro-abortion stance. What good does it do to mention exercise or alcohol while refusing to go near what has been found in studies around the world — abortion.
It’s also absurd to list family history as a risk factor — which is true but not preventable — while refusing to discuss abortion which is preventable.
It sounds unbelievable that groups claiming to be working against breast cancer are actually promoting breast cancer by not telling young women the full truth. But that’s exactly the situation.
Breast Cancer Hypocrisy Month
The closest either group comes to the abortion issue is Komen, mentioning breastfeeding as part of a healthy life for lowering risk: “Breastfeed if you can. Women who breastfeed have a lower risk of breast cancer than women who don’t breastfeed, especially before menopause. The longer a woman breastfeeds in her lifetime, the lower her risk may be.”
Correct. But why omit the significant factor of abortion if you really want to educate people?
BCRF lists these factors: weight/diet/exercise, alcohol use, smoking, timing of pregnancy, breastfeeding, and hormone use. Under ‘timing of pregnancy,’ we read, “giving birth later (after 30) or not having children can both increase a person’s breast cancer risk.” That’s as close as they get s to mentioning the drastic increase in risk after abortion. Yet they plead for donations: “Triple your impact for life-saving research during Breast Cancer Awareness Month!”
What’s the point of more research if they refuse to talk about the existing research?
Komen states: “Research clearly shows abortion (also called induced abortion) is not linked to an increased risk of breast cancer.”
That statement is false.
When Dr. Angela Lanfranchi, founder of the Breast Cancer Prevention Institute, attended medical school in the 1970s, women who got breast cancer were overwhelmingly older. As a breast surgeon, she saw younger women getting breast cancer and she became alarmed.
“I became concerned because I saw a lot of women in their 30s with breast cancer.” Lanfranchi shared with Human Life International. “None of them had a genetic reason… It was heartbreaking because all three had young children… so I started looking into risk factors.”
Research already showed that if you smoked and had a child, your risk of breast cancer increased 69%, but if you smoked and had no children, the risk increased 649%. What was it about having a child that protected women from getting breast cancer, Lanfranchi wanted to know.
 In 2023, JAMA published a study of U.S. cancers from 2010 to 2019. Women age 20-29 had a 5.3% increase in breast cancer and those 30-39 had a 19.4% increase in breast cancer. Shockingly, late stage, less curable breast cancer rate under age 40 has increased 3% per year over that time period. Young black women have almost five times the abortion rate as Caucasians and are suffering the greatest increases in breast cancer. These vulnerable women need early screening if their lives are to be saved. “
In 2023, JAMA published a study of U.S. cancers from 2010 to 2019. Women age 20-29 had a 5.3% increase in breast cancer and those 30-39 had a 19.4% increase in breast cancer. Shockingly, late stage, less curable breast cancer rate under age 40 has increased 3% per year over that time period. Young black women have almost five times the abortion rate as Caucasians and are suffering the greatest increases in breast cancer. These vulnerable women need early screening if their lives are to be saved. “
So the dramatic increase in breast cancer was noticed; what wasn’t cited was the causes that had already shown up in studies done since 1957.
In 1996, Dr. Joel Brind, endocrinologist and professor at Baruch College of the City University of NY, did a meta-analysis of all research on abortion and breast cancer and found confirmation.
Abortionists like Planned Parenthood emphasize the negatives of having a child, not the ramifications of abortion. The suppression of the truth is reinforced by the nation’s two largest breast cancer charities, leaving women in the dark about a growing disease by the very people who claim to be pro-woman.
The nation’s top abortion provider, Planned Parenthood, also promotes breast cancer awareness while denying the abortion connection. They use the month of October to fundraise, bragging that they offer breast exams while they profit from abortion.
How absurd is it to offer breast screening exams while simultaneously promoting breast cancer by selling abortion?
Time to Connect the Dots
BCPI’s Dr. Lanfranchi says the research from China is conclusive that breast cancer is the #1 risk factor for abortion.
China’s 1979 one-child policy led to an explosion of breast cancer. Forced and multiple abortions led to more screening for breast cancer as the rates and mortality increased greatly.
In 2019, the Chinese developed a risk model for Chinese women by conducting epidemiological studies to find the greatest risks in China. One study found a 151% increase risk with 1-2 abortions and a 530% increase in risk with three or more abortions. If women were over 30 years old when they had their first child, they had a 258% increased risk than women who were <25 years old when they had their first child.
Another study in 2022 found, “that when the rate of abortion rose, so did the risk of breast cancer. This association is biologically plausible as full-term pregnancy is a protective factor for breast cancer, and the breast enlarges due to the changing level of estrogen and progesterone during pregnancy. Immature breast cells are more likely to transform into breast cancer cells when the pregnancy is ended via abortion, which raises the risk of breast cancer.”
In fact, they found abortion was the greatest risk factor with a 613% increased risk for two or more abortions. About half of all U.S. women have repeat abortions.
Apparently, “Federal grant givers (NIH and NCI) are reluctant to publish data that might call into question the safety of abortion and hormonal contraception that is deemed essential to protect our planet from global warming and over-population,” Lanfranchi points out. “It’s ironic that in a country not known for freedoms [China], there was seemingly no problem in publishing data that could be seen as a criticism of public policy on abortion but not in the land of the free and the brave.”
Despite the dishonesty of many scientists in the U.S., the world’s scientific literature confirms the Abortion/Breast Cancer Link.
It’s disgusting that those profiting from abortion are using breast cancer to sell more abortions. The American Life league (ALL) cautions people against supporting these organizations.
Both earned negative ratings from the ALL’s Charity Watchlist, while the Breast Cancer Prevention Institute has a positive rating. ALL’s director Katie Xavios explained the most egregious concerns uncovered in researching these organizations.
“In 2024, a staggering 360,000 women across the nation are estimated to face the devastating diagnosis of breast cancer,” observed Brown. “The devaluation of human life as practiced by the Komen Foundation and the Breast Cancer Research Foundation compounds this tragedy. We urge donors who wish to support breast cancer prevention to consider charitable organizations that affirm and protect human life regardless of stage of development.”
“Life-minded donors seeking to support the fight against breast cancer will be pleased to discover that the Breast Cancer Prevention Institute (BCPI) upholds pro-life values and does not support anti-life organizations or agendas.”
Ivermectin’s Surprising Potential Against Cancer
Trump Warns His Patience With Putin Is “Running Out Fast”
Black Lives Matter Response to Iryna Zarutska’s Murder
DHS: Illegal alien fatally shot in Franklin Park after he attempted to drive car into ICE agents
Watching The End Game Of New York’s Climate Madness Begin To Play Out
Researchers Found Unvaccinated Children Healthier Than Vaccinated, Didn’t Publish Findings
Visualizing Americans’ Median Salaries By Age Group
AI, Inevitability, & Human Sovereignty
The Silent Soda Ingredient That Ages You from Inside
‘No Way’: Joe Biden Can’t Find Donors For His Presidential Library
Socialism Is the Problem, Not the Solution
Europe
Germany Just Noticed Renewable Energy has a Cybersecurity Problem
EU Nations Having Trouble Settling On A Climate (scam) Deal
MET OFFICE SHOCK: UK Temperature Network Goes From Bad to Even Worse in Just 18 Months
Charlie Kirk
NPR Turns to JERK Who Says Charlie Kirk Was a Racist Promoting ‘White Culture’ Against ‘Equity’
Erika Kirk Responds to Husband’s Assassination: ‘You Have No Idea the Fire You Have Ignited’
Vile Leftist BLASTED after attacking Erika Kirk for her remarks on the assassination of her husband
GEN Z IS COMING FOR YOU, YOU FUCKING TRAITORS!
No thanks asshole, I don’t want to die early. Could you just go away and stop ruining people’s lives?
Why we never want socialized medicine or the Government in our healthcare system.
My Wife’s Danish relatives love to say how their medical (among other things) is free. Well, it sucks. Every one of her relatives that had a procedure had it fucked up. They also had to wait 6 months to get anything done. They also pay 70% taxes to get the free medical care that sucks.
This one is about England, but socialized medicine is no good for anyone. They still haven’t repealed the ACA so our medical system is about as operative as the FAA right now. The US doctors are way better though.
An English professional boxer with a promising career ahead of her has tragically passed away, revealing the horror that is socialized medicine.
On May 22, the International Boxing Association issued a news release announcing that Georgia Cardinali, formerly known as Georgia O’Connor, had passed away at 25. She had been diagnosed with cancer in January, after seeking treatment for severe symptoms since October.
According to MMA Mania, Cardinali turned pro in 2021 after winning a gold medal at the 2017 Commonwealth Youth Games and a silver medal at the Youth World Championships that same year.
She was the youngest boxer ever to join the British team when she was 16.
She went on to compile a 3-0 professional record.
On May 9, just weeks before her death, she married her boyfriend, Adriano Cardinali.
News of her death is heartbreaking on its own, as this young athlete had everything to achieve in the sport, but her story is both devastating and infuriating when examined in the broader context of England’s socialized medicine program, the National Health Service.
On Jan. 31, Cardinali made a lengthy Facebook post, detailing how her doctors failed her in not diagnosing her cancer sooner, despite many warning signs and high risk factors.
The United States spends more on health care than any similarly large and wealthy country. However, in 2023, Americans had a life expectancy of 78.4 years, compared to an average of 82.5 among peer countries. This chart collection examines deaths in the U.S. and comparable countries through 2021, by age group and cause, to highlight factors that contribute to this life expectancy gap. The countries included in the comparison are Australia, Austria, Belgium, Canada, France, Germany, Japan, Netherlands, Sweden, Switzerland, and the United Kingdom.
The U.S.’s premature death rate (408 deaths per 100,000 people under age 70) in 2021 was almost twice the average of these similarly large and wealthy countries (228 deaths). About a third (32%) of the difference in premature death between the U.S. and similar countries is due to deaths from cardiovascular diseases, chronic respiratory diseases and chronic kidney diseases (which, combined, caused 105 deaths per 100,000 population under 70 in the U.S. in 2021). Additionally, in 2021, COVID-19 made up 24% of the difference in premature death rates between the U.S. and peer nations, killing 64 Americans out of every 100,000 under 70.
Another 12% of the difference between the U.S. and its peers’ premature death rates is due to substance use, which caused 29 deaths per 100,000 people under age 70 in the U.S. in 2021. For the purposes of this analysis, substance use deaths are defined as deaths occurring as a direct result of consumption of alcohol or illicit drugs, excluding any deaths from chronic diseases and organ damage caused by long-term use.
Deaths at younger ages bring down life expectancy more than deaths among older age groups. In the younger adult age group (15- to 49-year-olds), the difference in death rate between the U.S. and peer countries is largely driven by more deaths due to chronic diseases, COVID-19, and substance use. Among 15 to 49-year-olds, the U.S. death rate was 2.5 times that of comparable countries (192 vs. 76 per 100,000).
The charts below illustrate how among the under-70 population, the U.S. diabetes death rate is about 2.5 times that of comparable countries, the liver disease death rate is 1.6 times as high, and kidney disease death rate is 3.8 times as high. Additionally, the U.S. substance use death rate is four times that of comparable countries in the under-70 population, and the homicide death rate is nearly 8 times the average of peer nations.
click here for the rest and the charts
1

2
3
4

5

6
7
8
9
10
11
12

13

12
13
Choose an amount
Or enter a custom amount
Your contribution is appreciated.
Your contribution is appreciated.
Your contribution is appreciated.
DonateDonate monthlyDonate yearlyPretty soon, they won’t need men for anything.
I am beginning to feel intense pity for the regular citizens of the United Kingdom (UK).
Their leader is the absolutely horrendous Keir Starmer. Citizens can be tossed into jail for social media posts. Their electricity prices are soaring due to their leader’s green energy schemes.
Now there is another challenge that can be added to the list: Doctors in the UK are reporting a concerning increase in cases of necrotizing fasciitis of the vulva — a rare but extremely aggressive bacterial infection often called “flesh-eating disease.” This infection destroys soft tissue rapidly and can become fatal within hours if not treated promptly.
In a new case report published April 8 in the journal BMJ Case Reports, U.K. doctors describe three patients who were found to have necrotizing fasciitis of the vulva. The vulva includes the external female genitalia, such as the labia majora and labia minora, for example.
“Necrotizing fasciitis (NF), also known as flesh-eating disease, can arise when certain bacteria enter the skin through a wound — a cut, abrasion, burn, surgical wound, or even an insect bite,” Bill Sullivan, a professor of microbiology and immunology at Indiana University, who was not involved in the case report, told Live Science in an email. “NF can occur anywhere skin or tissue is breached, including genitalia.”
In necrotizing fasciitis, bacteria infiltrate the fascia, which is the connective tissue surrounding muscles, nerves, fat and blood vessels. The infection rapidly causes soft tissues to die, or “necrotize,” and spreads through the body very quickly.
A recent report from Shrewsbury and Telford Hospital NHS Trust detailed three women hospitalized with vulvar necrotizing fasciitis; one died less than 28 hours after diagnosis despite emergency surgery and intensive care.
In two of the cases, the women were diagnosed with vulvar necrotizing fasciitis in the emergency room. In the third, the woman developed it as a complication from an infected surgical wound.
One woman had seen a doctor five days earlier after noticing a spot on her mons pubis, and was prescribed antibiotics. But the treatment failed to clear the infection, and by the time she was hospitalized, the infection had spread throughout her labia majora, lower abdomen, and left hip. Despite surgical removal of her infected and necrotic tissue (also known as debridement) and intensive care support, the woman died of sepsis just 28 hours after her diagnosis.
The other two women survived their ordeal, though not without serious difficulty. Both needed “extensive surgical debridement” and one woman underwent three separate surgeries to remove tissue, which later required reconstructive surgery.
The hospital treated 20 cases between 2022 and 2024, surpassing the total number seen in the previous decade, indicating a concerning rise. Similar increases are being reported in other parts of Europe and the US, with invasive group A Streptococcus (the most common cause) infections doubling in the US between 2013 and 2022.
The number of invasive group A strep infections more than doubled from 2013 to 2022, according to a study from the Centers for Disease Control and Prevention published Monday in the Journal of the American Medical Association. Prior to that, rates of invasive strep had been stable for 17 years.
Invasive group A strep occurs when bacteria spread to areas of the body that are normally germ-free, such as the lungs or bloodstream. The same type of bacteria, group A streptococcus, is responsible for strep throat — a far milder infection.
Invasive strep can trigger necrotizing fasciitis, a soft tissue infection also known as flesh-eating disease, or streptococcal toxic shock syndrome, an immune reaction akin to sepsis that can lead to organ failure.
Girls, you need to learn how to keep that thing clean or we aren’t going to be able to service it.
UK Gynecologists Report Rise in Flesh-Eating Infections of the Vulva
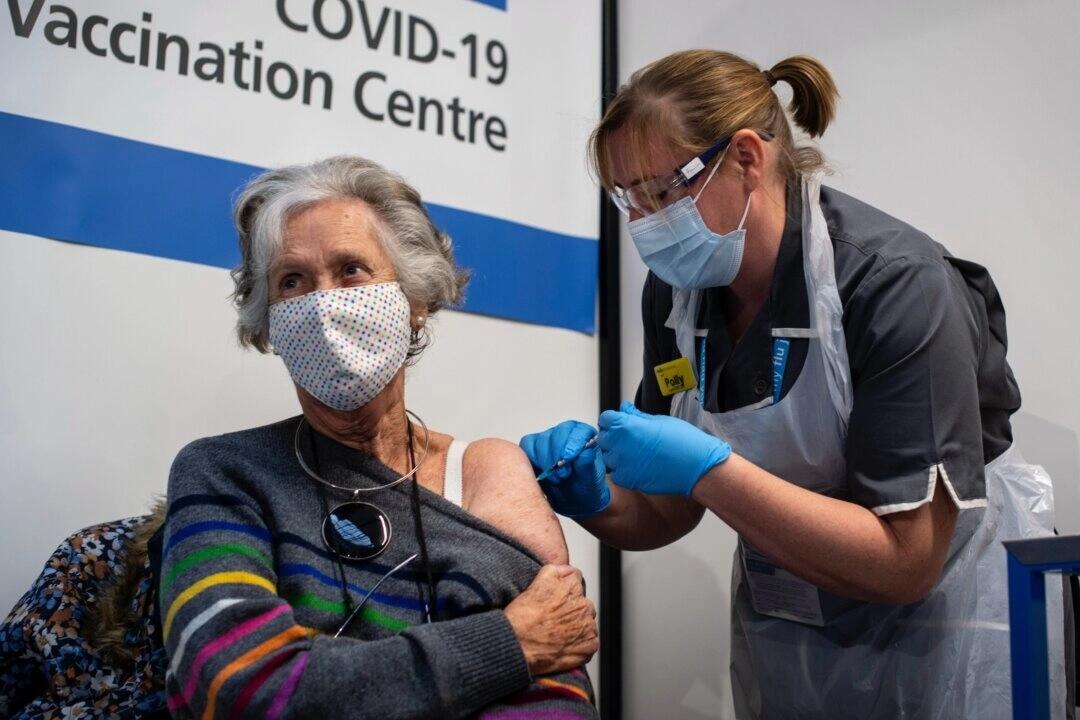
“Trust me, I’m a doctor” is a humorous expression that suggests one’s opinion should be accepted without question, regardless of whether the person offering the opinion has actual medical expertise or experience.
The assumption is that physicians are knowledgeable, competent, and trustworthy. At one time, few would have questioned that assumption.

Image via Grok
In 2013, Rasmussen Reports surveyed American adults and discovered that a significant majority, specifically 81%, trusted their doctor.
Four years later in 2017, that number was even higher, with 93% of patients trusting their regular doctor.
A funny thing happened in late 2019 and early 2020. In late 2019, almost no one had ever heard of COVID, coronavirus, or Wuhan.
The World Military Games were held, of all places, in Wuhan, China, in October 2019. A Department of Defense report from 2022 suggested that seven military members might have become infected with COVID-19.
We are only hearing about this now, two and a half years later. Apparently, this report was concealed among the Epstein files or Hunter Biden’s and Anthony Weiner’s laptops. However, the Biden administration covered up this report, just as they obscured their boss’s mental state and cognitive decline for four years.
Lies and coverups are a great way to destroy trust.
Dr. Anthony Fauci and his cabal lied to the public about the origins of COVID with their nonsensical “proximal origin” theory.
Why? To discredit President Donald Trump, who blamed China, and to conceal their illegal gain-of-function research.
Additionally, it may have been to maintain and protect money flow from China to the pharma-industrial complex.
This is one reason why trust in doctors and the medical profession has declined sharply over the past five years. You don’t have to take my word for it; I live and work in this new world of dwindling trust and observe it all around me.
The Journal of the American Medical Association conducted a survey of nearly half a million American adults across all 50 states and found, “The COVID-19 pandemic has been associated with a continuing decrease in trust in physicians and hospitals, which may necessitate strategies to rebuild that trust to achieve public health priorities.”
The Wall Street Journal, taking a break from criticizing President Trump over immigration and tariffs, noticed the declining trust in doctors. This past February, they published an article questioning, “Why we don’t trust doctors like we used to.”
They referenced a Gallup survey that stated, “Americans’ ratings of US professions stay historically low.”
In other words, it’s not only doctors who are held in low esteem but much of the administrative class as well.
Interestingly, another group of healthcare professionals topped the list, “Three in four Americans consider nurses highly honest and ethical, making them the most trusted of 23 professions rated in Gallup’s annual measurement.” Those surveyed must have missed the incessant TikTok videos of nurses dancing in ICUs during COVID.
And to no surprise for anyone engaged in politics and the news, “The least trusted professions, with more than half of U.S. adults saying their ethics are low or very low, are lobbyists, members of Congress and TV reporters.”
But it’s doctors falling most rapidly from grace, “About 53% of those polled in 2024 gave a high or very high rating to medical doctors, down from 67% in 2021. It’s the biggest drop among 23 professions ranked by Gallup in that period.”
There are many reasons. The WSJ offered a partial explanation:
People are increasingly wary of a healthcare system that is supposed to make them feel better but instead leaves them stressed and frustrated. And while much ire is directed at insurance and pharmaceutical companies, doctors are the front face of the system and are losing the public’s confidence, as well.
However, they overlooked the elephant that entered the room in late 2019, an elephant named COVID.
Consider the business and school lockdowns that closed churches while allowing strip clubs and liquor stores to remain open. It was illegal to surf alone in the Pacific Ocean, yet thousands marching together on city streets in the name of BLM or Antifa were considered perfectly safe and healthy.
Masks were deemed ineffective at protecting against tiny viruses until they were mandated as effective and lifesaving. As Dr. Anthony Fauci acknowledged, social distancing was arbitrary; “It sort of just appeared.” How’s that for science? As Gomer Pyle would say, “Shazam, shazam!”
The vaccines proved to be neither safe nor effective. Otherwise, we wouldn’t be hearing about sudden deaths, blood clots, or myocarditis. Additionally, those vaccinated and boosted would not continue to contract COVID. Or as a Cleveland Clinic study found, the chance of getting COVID increased with an increasing number of vaccine doses and boosters.
Children lost years of education and social interaction to avoid catching a viral illness that posed virtually no risk of death to children. Jobs, businesses, and livelihoods were devastated due to political motivations rather than medical science. What impact does this have on trust in the medical system?
The U.S. healthcare system is failing Americans. The Commonwealth Fund reports, “The US spends the most on healthcare but has the worst health outcomes among high-income countries.” In most businesses, this would signal a death knell.
Then, there is the dysfunctional medical payment system, a combination of government and corporate control, which separates patients as consumers from physicians and hospitals as providers.
The Medicare fee schedule, which serves as the basis for all third-party insurance payments, will reduce reimbursement by 3% in 2025. This marks the fifth consecutive year of payment reductions, even as the cost of providing care continues to rise.
Physicians are compelled to see more patients throughout their workday, which results in spending less time with each individual and longer waits for appointments or to see the doctor during a brief office visit.
Patients are understandably frustrated and now see a doctor’s visit similar to a DMV trip.
The loss of trust extends beyond doctors; it includes the entire healthcare system, encompassing government-run health agencies and insurance companies.
The public has been overwhelmed by a continuous influx of misinformation, especially concerning the COVID pandemic, and has encountered censorship for asking questions or expressing complaints. Americans have been made to believe that our healthcare system is the best.
Although the system may benefit certain patients in particular situations, we fail spectacularly on a population level. Practicing medicine is no longer a calling or profession; instead, it has become a people-facing service trade influenced by price controls and an increasing number of rules and regulations.
Any private sector business operating in such a manner would quickly go out of business.
Trust lost is difficult to regain. Through transparency and disclosure, Robert F. Kennedy, Jr. may step in the right direction.
However, the basic structure of the healthcare delivery system is deeply flawed, and elected officials have no interest in undertaking the major reforms necessary to right the ship.
Healthcare spending in the U.S. exceeds $5 trillion, accounting for 18% of GDP, and continues to grow each year. Meanwhile, life expectancy in the U.S. is declining, and chronic diseases are on the rise.
Physicians who observe and voice any concerns may face censorship or threats to their medical licenses or employment. I experienced such backlash from the medical-industrial complex during the pandemic.
Clearly, what we are doing is not working, yet we are following the definition of insanity — doing the same thing repeatedly and expecting a different result.
It’s no surprise that fewer Americans trust the healthcare system. The phrase “Trust me, I’m a doctor” is fading into obscurity like another ridiculous saying from the past: “More doctors smoke Camels than any other cigarette.”
We must be able to trust our doctors with our lives and well-being. Can we still do that?
“The risk of integration of synthetic mRNA-based gene therapies and/or associated DNA fragment adulterants into the human genome of either somatic or germ cells are uncharacterized,” the legislation explains, adding that any germline integration “creates risk of random human genomic modifications being passed on to the next generation of Americans.”
South Carolina lawmakers have introduced a bill that would ban healthcare professionals from administering synthetic mRNA-based gene therapies, including COVID-19 vaccines, citing contamination, long-term safety concerns, and the risk of genetic damage to future generations.
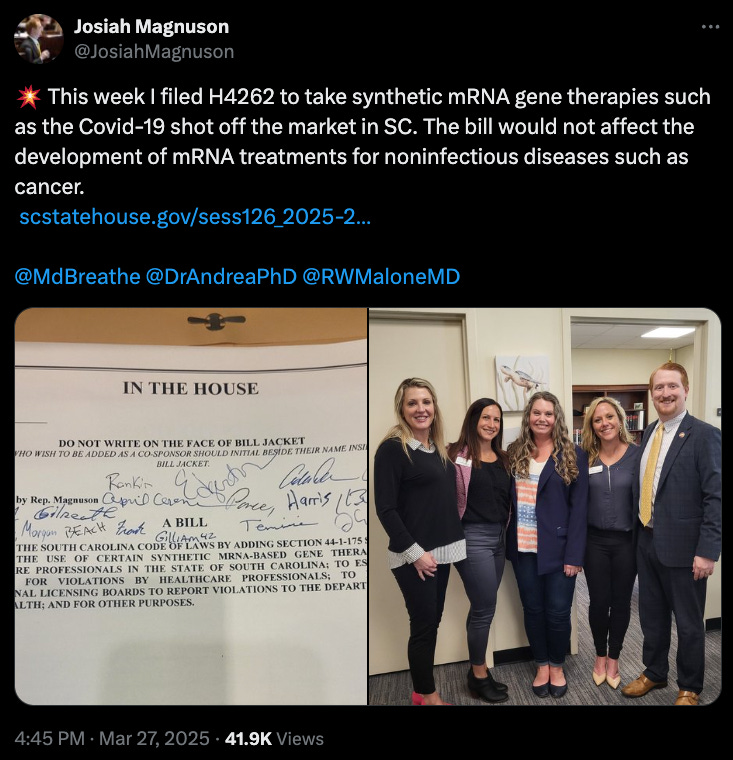
Dr. Mary Talley Bowden, whose groundbreaking lawsuit forced the FDA to remove its anti-ivermectin social media posts in March 2024, celebrated the move.
“Add South Carolina to the list of states calling for an end to Covid mRNA shots,” she wrote in an X post.
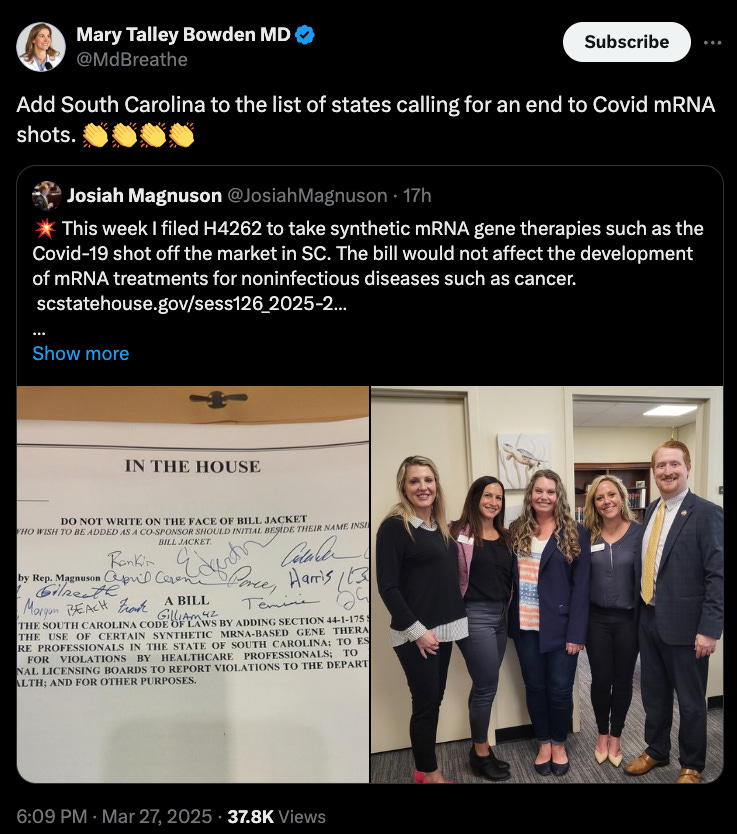
HB 4262, introduced March 27, 2025, by Reps. Magnuson, Rankin, Edgerton, Duncan, Kilmartin, Cromer, and more than a dozen other co-sponsors, would amend the South Carolina Code to prohibit the use of certain mRNA products and impose strict penalties on violators.
“Synthetic messenger ribonucleic acid (mRNA)-based gene therapies, such as the COVID-19 vaccine, have caused substantial numbers of deaths, disabilities, and a wide range of serious adverse events,” the bill states.
The bill affirms mRNA-based products are “contaminated with DNA fragments, metallic particles, and other undisclosed and/or otherwise poorly characterized adulterants.”
It warns that no long-term studies have been completed on shedding, fertility, teratogenicity, mutagenicity, or cancer risk.
“The risk of integration of synthetic mRNA-based gene therapies and/or associated DNA fragment adulterants into the human genome of either somatic or germ cells are uncharacterized,” the legislation explains, adding that any germline integration “creates risk of random human genomic modifications being passed on to the next generation of Americans.”
The measure blasts the lack of informed consent for recipients, pointing out that individuals are “not provided adequate information both as to the nature of the harm posed to them” and that they’re barred from seeking compensation under current federal law.
“Therefore,” the bill states, they “do not have the ability to give valid consent to have medical products employing this material or the delivery procedure administered.”
Significantly, lawmakers assert that the spike proteins in mRNA COVID shots may “be communicable to others (by a process known as ‘shedding’) and may cause side effects or harm even in individuals who are not the intended recipient.”
HB 4262 would strictly prohibit healthcare professionals from administering any “synthetic mRNA-based gene therapy product” within the state, unless used to treat noninfectious diseases such as cancer or rare genetic disorders.
It defines “synthetic mRNA-based gene therapy” as any product that introduces foreign genetic material into human cells to exert medical effects through transcription, translation, genomic integration, or genetic modification.
This includes:
Violating the proposed law would carry harsh penalties:
“Intentional or wilful violation… shall result in a suspension of the healthcare professional’s license… for no less than one year,” the bill states. Licensing boards could also apply additional penalties and fines at their discretion.
Licensing boards would be required to report any violations to the Director of the Department of Public Health, who must:
“Keep record of the violations for no less than seven years and… inform the General Assembly of the number and nature of violations no less than annually.”
The legislation was introduced and read for the first time in the South Carolina House on March 27 and was referred to the Committee on Medical, Military, Public and Municipal Affairs.
If passed and signed into law, the act would take effect immediately upon approval by the Governor.
The bill can be read in full here.
With South Carolina now taking the lead, HB 4262 marks a bold legislative stand against what lawmakers call an “inadequately characterized potential public health threat”—and it could become the blueprint for other states ready to draw the line.
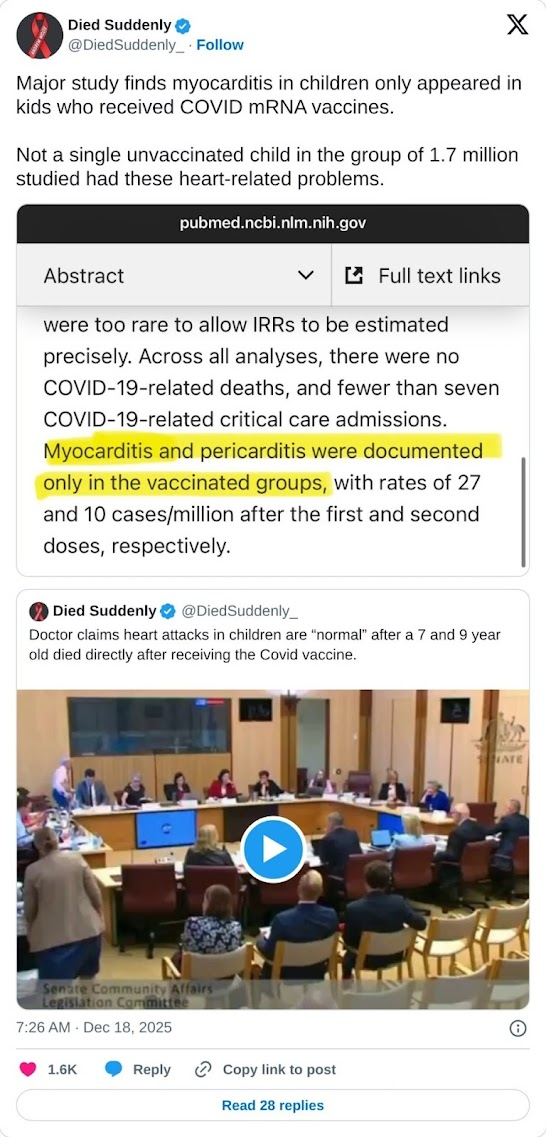
A major peer-reviewed study of almost 100 million people has confirmed that Covid mRNA “vaccines” have caused a global surge in death and deadly disease.
The study documents the outcomes of 99 million people after they received Covid mRNA injections.
During the study, the researchers examined the official government data from eight countries.
Participants in the study included 99,068,901 Covid-vaccinated individuals.
The study has concluded that the injections are responsible for the global surge in sudden deaths and life-threatening illnesses.
The researchers found that staggering numbers of vaccinated people suffered serious complications such as heart failure, blood clots, strokes, brain disorders, and severely weakened immune systems.
Many of those tracked by the peer-reviewed study also died suddenly and unexpectedly.
The research was conducted by the Global Vaccine Data Network in New Zealand.
The study’s paper was published in the prestigious, world-renowned Vaccine journal.
Two decades ago, CBS aired a bombshell report on the flu shot, revealing a truth that health officials didn’t want to admit. Despite flu shot uptake among seniors skyrocketing from 15% to 65%, flu deaths continued to climb. It doesn’t fucking work and the whole thing is a farce.

NIH scientists were devastated. They expected the data to confirm the vaccine’s effectiveness. But instead, their own research shattered that assumption. So they assumed other factors must be “masking the true benefits of the shots.”

Image Credit: Shutterstock / Mr. Nikon
However, as
Sharyl Attkisson reported at the time, “No matter how they crunched the numbers, they got the same disappointing result. Flu shots have not reduced deaths among the elderly.”
Atkisson, the reporter in the above clip, later left mainstream news to become an independent journalist focused on exposing Big Pharma, government corruption, and mainstream media lies.
Going back to the story, the scientists looked at the flu shot data of other countries in hopes of finding more optimistic data. But what they found instead was “the same poor results in Australia, France, Canada, and the UK.”
Family members of those harmed by vaccines told the UK Covid-19 Inquiry they were forced to form their own support systems after being ignored by the authorities and made to feel like “an uncomfortable truth” of the rollout.
Kate Scott, speaking on behalf of the group Vaccine Injured and Bereaved UK (VIBUK), said they felt they were “almost being pushed into the shadows” as the overwhelming official message continued to be that the jabs were ”safe and effective” in spite of their experience.
Last week’s hearing also heard from a victims’ group in Scotland which raised concerns that the vaccine had been rolled out at such speed that public safety had been sacrifice
Module 4 of the long-running inquiry, chaired by Baroness Heather Hallett, is examining issues relating to the development of COVID-19 vaccines and other drugs.
Scott, whose husband Jamie was left severely disabled by the vaccine, said:
“We are an uncomfortable truth, but we are a truth, and the truth is for everyone in our group, the vaccine caused serious harm and death.”
Jamie Scott spent over a month in a coma after suffering the life-threatening side effect known as vaccine-induced immune thrombosis and thrombocytopenia after taking the now withdrawn AstraZeneca jab.
He survived but with a serious brain injury which has left him unable to work, partially blind, and unable to live independently, while his wife also had to give up her job to help care for him.
He received the maximum payout of £120,000 from the government’s Vaccine Damage Payment Scheme (VDPS) which is given to those who are assessed as being left 60 percent disabled as a result of a vaccine.
The inquiry will consider whether the VDPS should be reformed after some vaccine-injured people were left without the payment because they were assessed as not being severely disabled enough, even when left with life-changing health problems.
Kate Scott said, “The scheme is inadequate, insufficient, and offers too little too late and to too few.”
She told the hearing that victims of vaccine damage were made to feel that were “the only ones, or the unlucky ones, and just get on with it, and that’s impossible when you’re grieving a loved one, or your husband is in intensive care.”
A Freedom of Information request made by VIBUK showed that, as of November 2024, victims or their family members have made 17,519 claims to the scheme.
They bought the safe and effective lie and are now paying the price
Americans don’t trust public health institutions, the virologist who used to head the Centers for Disease Control and Prevention says.
“We have lost public trust, there’s no doubt about it, and it really harms public health in a big way,” Robert Redfield said Wednesday during an event at The Heritage Foundation, adding, “We’ve lost, I think, trust in science.”
The lines between public health institutions and politics became blurred during the pandemic, Kulldorff said.
The National Institutes of Health is a government research agency and “their role is not policy or public health policy,” he said.
Yet, Dr. Anthony Fauci, who directed the National Institute of Allergy and Infectious Diseases for nearly four decades until 2022, became quite involved in health policy while an adviser to two presidents during the pandemic.
NIH “should have focused on doing the studies to find out, for example, about genetic drugs, if they can help against COVID,” Kulldorff said. But instead, he added, Fauci “sort of took over that public health policy, which doesn’t make any sense.”
Schools shouldn’t have been closed and lockdowns shouldn’t have been widespread, Kulldorff said, but the “biggest chunk of the infectious disease research money was controlled by Dr. Fauci, so he took a very active role about the pandemic policy.”
Instead of a health system, Americans “pay for illness,” Redfield said, adding: “As long as you’re sick, the system works. We need to flip the switch … so that we pay for wellness.”
One of the “root causes” of the public health crisis is that doctors are “at the bottom of the treatment pyramid,” Johnson said.
Doctors “should be at the top,” he said, but are being “crushed by the agencies” in a third-party payer system in America.
how many times can a bartender piss in a mug and keep telling you it’s a beer? That’s what the government is doing to us
To begin with, it’s a Marxist idea and very few ideologies in history have killed more people than Marxism.
Specifically, this is what is happening.
I’m old enough to remember when health insurance was affordable. It wasn’t all that long ago; it was before Obamacare passed. Despite being officially called the Affordable Care Act, nothing about it has made health insurance more affordable. The question is, for the higher premiums and larger deductibles we have, are we even getting better coverage? The answer, which shouldn’t shock you, is a big fat “no.”
That’s right, despite paying more, you are also getting less. Health insurance denials and delays have hit record highs, and while many point the finger at insurance companies, accusing them of prioritizing profits over care, they’re not to blame. As Betsy McCaughey points out, the real culprits are the politicians who sold us Obamacare on a pile of lies.
“In 2013, before Affordable Care Act regulations kicked in, insurers denied roughly 1.5% of claims, according to the American Medical Association,” McCaughey points out. “But under ACA rules, denials increased tenfold. Now nearly 15% of claims are denied,” and some insurers are denying a third or more of claims.
Doctors and patients aren’t just battling denials — they’re also tangled in a bureaucratic nightmare of preauthorizations. As McCaughey notes, these delays force doctors to get insurer approval before providing care. And here’s the kicker: the person giving the green light is often unqualified to make those decisions. The AMA warns that an OB-GYN might be the one overriding your neurosurgeon’s recommended treatment.
And the consequences can be deadly.
McCaughey cites the example of a doctor who had a patient with metastatic breast cancer who needed a specific drug combination. But thanks to prior authorization delays, she had to settle for standard chemotherapy, which failed, and the patient died.
Obamacare is killing people.
It’s not just anecdotes. A House Committee on Energy and Commerce investigation found that Cigna overturned 80% of its Medicare Advantage preapproval denials upon appeal, proving that legitimate care is being withheld. And, as McCaughey reports, Cigna’s algorithm, PxDx, denies authorizations in bulk without considering individual cases.
If you like your doctor, you can keep your doctor. If you like your plan, you can keep your plan. That and everything else that came out of his mouth was an effing lie.
My wife’s dumbass relatives in Denmark can’t brag enough to me about their free healthcare, to which I say you pay 70% taxes, so it’s not free. They try to make America into Denmark and what sort of works for 5 million doesn’t translate to 330+ million. They don’t get it because they mostly want to trash the US. Plus, they are socialist and we’re not.
Well, here’s the facts. It doesn’t work, the doctors are crummy, you have to wait for months and you can’t sue for malpractice, which at least 4 of her relatives have received for healthcare and are now injured.
Now this story:
Advocates for “universal health care” love to use Finland as an example of a system that works. That is an absurd comparison. Finland has a culturally homogeneous population of 5.6 million; that is just over half the population of Los Angeles County (9.6 million).
Better examples are England and Canada.
England has government-funded “universal health care” in the form of the National Health Service. The population of England is around 57 million people. Wait times for nonemergency care average 14 to 18 weeks, and thousands of people have been waiting more than 18 months. As of June of this year, 7.5 million Brits were waiting for already scheduled procedures and surgeries requiring hospital stays, more than 300,000 of whom had been waiting for more than a year.
Keep in mind that these scheduled – and delayed – procedures include diagnostic tests and treatments for illnesses like cancer. Shortages of physicians and treatment facilities force cancer patients to wait weeks – or months – for radiation or chemotherapy.
These delays have life-and-death consequences. In 2009, British medical journal Lancet reported that 51.1% of British cancer patients were alive five years after their diagnosis. By contrast, 91.9% of American cancer patients were alive five years after their diagnosis.
England’s problems are not limited to cancer care. Last year, Bloomberg News published a report analyzing the NHS’s own data. The results were shocking. In most areas of England, medical care failed to meet government goals in things as basic as minimum wait times for an ambulance to arrive in an emergency (goal: 30 minutes; reality: up to three hours) or the availability of hospital beds.
In Canada – another country with “universal health care,” the situation is nearly as bad. Canada has a population of nearly 40 million. The average wait time for treatment in Canada for a condition requiring a specialist’s care is more than six months. But in some provinces and for some procedures – like orthopedic surgery or neurosurgery – the wait is closer to a year, or even longer. Canadians face long waits – six weeks to three months – even for simple but vital diagnostic procedures like MRIs, CT scans or ultrasounds.
By contrast, in the United States – a country with 330 million people – the average wait time for a nonemergency appointment with a specialist is only 26 days (a situation that medical journal STAT called “a public health crisis”). The median time between diagnosis of cancer and commencement of treatment is 27 days. The average wait time for an ambulance here is seven minutes.
So here’s the deal – remember when “experts” kept telling us what to do during COVID?
Turns out they got pretty much everything wrong. Like, spectacularly wrong.
We’re talking 19 major things they completely screwed up, from how the virus spreads to whether masks actually work (spoiler alert: those cloth masks were basically fashion accessories).
Dr. Fauci is the patron saint of TERRIBLE COVID policies.
He was wrong on SO MANY POINTS. It’s time to set the record straight…
Did he get anything right?
Last year the Norfolk Group just dropped a bomb of a document laying out all these failures. And it’s not just Monday morning quarterbacking – they’ve got the receipts. Real studies showing how natural immunity was actually legit (while Fauci pretended it didn’t exist), data proving schools could’ve stayed open (looking at you, Sweden), and evidence that maybe, just maybe, locking healthy people in their homes wasn’t the brilliant strategy they claimed.
Listen, I’m not here to say “I told you so” (okay, maybe a little), but we need to talk about this. Because if we don’t learn from how badly our “experts” messed up, we’re just asking for a repeat performance next time around. And honestly? I don’t think any of us can handle another round of plexiglass theater and double masking.
Let’s break down exactly how they got it wrong, and more importantly, why they kept doubling down even when the evidence said otherwise. Buckle up – this is gonna be a wild ride through the greatest public health face-plant in modern history.
These are the questions WE want answered!
Screw the old people who need help. Kick the Medicare can down the road, but make sure to fund a climate scam that launders money to politicians.
When Democrats rammed through the Inflation Reduction Act during the days they controlled all of Washington, D.C., it ignited a chain reaction that led to higher Medicare costs for America’s senior citizens.
“Nearly two years after its passage, the IRA has diverted nearly $260 billion from the projected Medicare ‘savings’ to pay for special interest handouts like large tax credits for costly electric vehicles, enormous subsidies paid to big health insurer-PBM corporations, and funding health care programs for illegal immigrants,” Ron Fitzwater, Chief Executive Officer of the Missouri Pharmacy Association, wrote in an Op-Ed in the Missouri Times.
“The Biden-Harris administration is not protecting Medicare; they’re stealing from it,” he wrote.
According to Politico, the chain reaction began when the act shifted the burden of paying for prescription medicine from seniors to insurance companies.
Then came what could have been predicted: Insurance companies hiked their premiums for 2025.
Fitwater, in his Op-Ed, said increases were coming in at 179 percent.
But since that was going to hit right before the election, there was one more step – a federal bailout that has the taxpayer-funded federal treasury taking the hit for what the IRA caused.
Now, in something cool…
Advancements in technology are continually reshaping the landscape of mobility aids, particularly for individuals with disabilities. Among these innovations, the WalkON Suit F1, developed by KAIST (Korea Advanced Institute of Science and Technology), stands out as a groundbreaking solution for paraplegic patients. Let’s delve into the features, development, and implications of this remarkable wearable robot.
Imagine an exoskeleton that doesn’t just help you walk—it comes to you. That’s right, the WalkON Suit F1 can actually walk over to a person in a wheelchair. This incredible piece of tech solves a major problem that other exoskeletons face. You see, most exoskeletons require helpers to lift users out of their wheelchairs and strap them in. But the WalkON Suit F1? It’s got a nifty front-docking system that lets the person put it on while still seated in their wheelchair. Talk about independence.
The suit features a system “that actively controls the center of its weight against the pull of gravity” to prevent it from toppling over as the person stands up. And get this—the WalkON Suit F1 has been tweaked to allow people to use both hands while standing upright and even take short walks without needing a cane.
Many chronic diseases can be traced to mitochondrial dysfunction, according to Chen Junxu, a natural medicine expert at Bastyr University. After reviewing over 500 research papers and drawing from his extensive clinical practice, Chen developed a comprehensive theory about the relationship between mitochondrial health and chronic disease, which he shared in a recent interview on NTDTV’s “Health 1+1“ program.
Mitochondria are often called the power generators of human cells. They convert nutrients such as glucose and fatty acids that we obtain from food into adenosine triphosphate (ATP), the primary energy source in our cells during metabolism.
At the same time, mitochondria are the core of human immunity, too. Healthy mitochondria effectively regulate immune responses, while mitochondrial dysfunction can damage immune cells, resulting in many chronic diseases and impaired cellular differentiation.
Chen argues that seemingly diverse conditions—including diabetes, hypertension, heart disease, cancer, allergies, autoimmune diseases such as rheumatoid arthritis, and even various mental illnesses—can be understood through a “unified theory” of mitochondrial imbalance. This means that almost every disease can be traced to mitochondrial imbalance. In other words, in mitochondrial imbalance, there is invariably something wrong with the body’s basic metabolism. This perspective suggests that approximately 90 percent of chronic diseases stem from problems with mitochondrial metabolism.
About 18,000 Americans are diagnosed with a new case of oropharyngeal cancer each year, with a UK head, neck and thyroid surgeon pointing the finger at oral sex.
Oropharyngeal cancer is a type of head and neck cancer that tends to affect people between 50 and 80 but is becoming more prevalent among younger generations because it’s linked to human papillomavirus (HPV).

“HPV is sexually transmitted. For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” Dr. Hisham Mehanna, a professor at the University of Birmingham in the UK, wrote Monday on the Conversation research site.
“Those with six or more lifetime oral sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex,” Mehanna added.
The cancer strikes the middle portion of the throat, behind the mouth. That area includes the soft palate, tonsils, back of the tongue and the sides and back of the throat.
It’s how Michael Douglas got it. I’m not calling a moratorium on BJ’s yet. I still have a few more that I’d like to get from girls.
It’s going to be tough on the lesbians.
With the entire Media propaganda machine working against him, here’s the other side of the coin for fairness’ sake. Ackman is a heavyweight investor, worth listening to whether you agree with him or not.
Prominent hedge fund manager Bill Ackman provided one of the best lists of reasons to vote for Donald Trump. What would you do differently if you wanted to destroy the United States?
While the 33 actions I describe below are those of the Democratic Party and the Biden/Harris administration, they are also the actions and policies that, unfortunately, our most aggressive adversaries would likely implement if they wanted to destroy America from within and had the ability to take control of our leadership.
(1) open the borders to millions of immigrants who were not screened for their risk to the country, dumping them into communities where the new immigrants overwhelm existing communities and the infrastructure to support the new entrants, at the expense of the historic residents,
(2) introduce economic policies and massively increase spending without regard to their impact on inflation and the consequences for low-income Americans and the increase in our deficit and national debt,
(3) withdraw from Afghanistan, abandoning our local partners and the civilians who worked alongside us in an unprepared, overnight withdrawal that led to American casualties and destroyed the lives of Afghani women and girls for generations, against the strong advice of our military leadership, and thereafter not showing appropriate respect for their loss at a memorial ceremony in their honor,
(4) introduce thousands of new and unnecessary regulations in light of the existing regulatory regime that interferes with our businesses’ ability to compete, restraining the development of desperately needed housing, infrastructure, and energy production with the associated inflationary effects,
(5) modify the bail system so that violent criminals are released without bail,
6) destroy our street retailers and communities and promote lawlessness by making shoplifting (except above large thresholds) no longer a criminal offense,
(7) limit and/or attempt to limit or ban fracking and LNG so that U.S. energy costs increase substantially and the U.S. loses its energy independence,
(8) promote DEI ideologies that award jobs, awards, and university admissions on the basis of race, sexual identity and gender criteria, and teach our students and citizens that the world can only be understood as an unfair battle between oppressors and the oppressed, where the oppressors are only successful due to structural racism or a rigged system and the oppressed are simply victims of an unfair system and world,
(9) educate our elementary children that gender is fluid, something to be chosen by a child, and promote hormone blockers and gender reassignment surgeries to our youth without regard to the longer-term consequences to their mental and physical health, and allow biological boys and men to compete in girls and women’s sports, depriving girls and women of scholarships, awards, and other opportunities that they would have rightly earned otherwise,
(10) encourage and celebrate massive protests and riots that lead to the burning and destruction of local retail and business establishments while at the same time requiring schools to be shuttered because of the risk of Covid-19 spreading during large gatherings,
(11) encourage and celebrate anti-American and anti-Israel protests and flag burning on campuses around the country with no consequences for the protesters who violate laws or university codes and policies,
(12) allow antisemitism to explode with no serious efforts from the administration to quell this hatred,
(13) mandate vaccines that have not been adequately tested nor have their risks been properly considered compared with the potential benefits adjusted for the age and health of the individual, censoring the contrary advice of top scientists around the world,
(14) shut down free speech in media and on social media platforms that is inconsistent with government policies and objectives,
(15) use the U.S., state, and local legal systems to attack and attempt to jail, take off the campaign trail, and/or massively fine candidates for the presidency without regard to the merits or precedential issues of the case,
(16) seek to defund the police and promote anti-police rhetoric causing a loss of confidence in those who are charged with protecting us,
(17) use government funds to subsidize auto companies and internet providers with vastly more expensive, dated and/or lower-quality technology when greatly superior and cheaper alternatives are available from companies that are owned and/or managed by individuals not favored by the current administration,
(18) mandate in legislation and otherwise government solutions to problems when the private sector can do a vastly better, faster, and cheaper job,
(19) seek to ban gas-powered cars and stoves without regard to the economic and practical consequences of doing so,
(20) take no serious actions when 45 American citizens are killed by terrorists and 12 are taken hostage,
(21) hold back armaments and weaponry from our most important ally in the Middle East in the midst of their hostage negotiations, hostages who include American citizens who have now been held for more than one year,
(22) eliminate sanctions on one of our most dangerous enemies enabling them to generate $150 billion+ of cash reserves from oil sales, which they can then use to fund terrorist proxy organizations who attack us and our allies. Exchange five American hostages held by Iran for five Iranians plus $6 billion of cash in the worst hostage negotiation in history setting a disastrous and dangerous precedent,
(23) remove known terrorist organizations from the terrorist list so we can provide aid to their people, and allow them to shoot rockets at U.S. assets and military bases with little if any military response from us,
(24) lie to the American people about the cognitive health of the president and accuse those who provide video evidence of his decline of sharing doctored videos and being right wing conspirators,
(25) do nothing about the deteriorating health of our citizens driven by the food industrial complex, the fraudulent USDA food pyramid, and the inclusion of ingredients in our food that are banned by other countries around the world which are more protective of their citizens,
(26) do nothing about the proliferation of new vaccines that are not properly analyzed for their risk versus the potential benefit for healthy children who are mandated to receive them,
(27) do nothing about the continued exemption from liability for the pharma industry that has led to a proliferation of mandatory vaccines for children without considering the potential cumulative effects of the now mandated 72-shot regime,
(28) convince our minority youth that they are victims of a rigged system and that the American dream is not available to them,
(29) fail to provide adequate Secret Service protection for alternative presidential candidates,
(30) litigate to prevent alternative candidates from getting on the ballot, and take other anti-competitive steps including threatening political consultants who wish to work for alternative candidates for the presidency, and limit the potential media access for other candidates by threatening the networks’ future access to the administration and access to ‘scoops’ if they platform an alternative candidate,
(31) select the Democratic nominee for president in a backroom process by undisclosed party leaders without allowing Americans to choose between candidates in an open primary,
(32) choose an inferior candidate for the presidency when other much more qualified candidates are available and interested to serve,
(33) litigate to make it illegal for states to require proof of citizenship, voter ID, and/or residence in order to vote at a time when many Americans have lost confidence in the accuracy and trustworthiness of our voting system.
Health-benefit costs are expected to exceed salary increases despite the Biden-Harris administration claiming to have helped redress the issue, a study from advisory firm Mercer found.
Employer-provided health insurance expenses rose 7% in 2024 and are expected to rise 5.8% in 2025, with over half of the 1,800 employers surveyed telling Mercer they plan to cut insurance plan costs in the new year, often through increasing out-of-pocket costs for employees. The increase in healthcare expenses is expected to outpace salary growth, with performance-based raises and total salary budgets predicted to rise just 3.3% and 3.6% next year, respectively.
Prescription drug spending is the fastest-growing component of the surge in health-benefit costs, rising 7.2% in 2024 and expected to continue increasing in 2025 due to new high-cost gene and cellular therapies, according to Mercer. Rising healthcare costs are also largely driven by a growing disparity between the supply of healthcare workers and a rising demand for medical services as older Americans become an increasingly large segment of the population.
The Biden-Harris administration claimed it would address rising healthcare costs, vowing
in March to reduce premiums by an average of $800 a year for millions
of Americans by expanding Affordable Care Act tax credits. The White
House also capped prescription drug costs at $2,000 per year for
Medicare beneficiaries starting in 2025 — a move that experts told
the Daily Caller News Foundation would have caused a spike in Medicare
premiums if not for the administration providing billions in subsidies
for insurers in a ploy to buy votes.
A renowned American physician is sounding the alarm over skyrocketing numbers of young people being diagnosed with deadly cancers.
Dr. Cynthis Yoshida, a professor at the University of Virginia (UVA), warns that this troubling trend has now “become an epidemic.”
Yoshida, who leads UVA’s Health Cancer Center’s Colorectal Cancer Screening Program, is now alerting the public via local media outlets.
Scientists, physicians, and oncologists around the world have been reporting that cancer cases have spiked dramatically since 2021.
During an interview with Charlottesville’s 29News, Dr. Yoshida expressed her concerns.
“It’s really become an epidemic,” Yoshida warned.
“When my patients come in and have the colonoscopies, so many more are asking, ‘What is it that’s causing this rise in early onset cancers?’”
According to Dr. Yoshida, every year 18,000 people under the age of 50 are diagnosed with early-onset cancer.
However, the cancers are spreading so rapidly that often these individuals are diagnosed too late to survive.
What a prick. Screwing the public while screwing around, completely doing the opposite of what he was making the public do. They all knew Covid-19 was a hoax.
Dr. Jay K. Varma, New York City’s former top public health advisor during the pandemic, was caught on camera bragging about attending drug-fueled sex parties and dance events, even as he instructed millions of New Yorkers to stay home and socially distance. The bombshell revelations have sparked outrage across the city, with politicians and residents alike accusing the former official of blatant hypocrisy.

The footage, released Thursday by conservative podcaster Steven Crowder, shows Varma, who served under then-Mayor Bill de Blasio, detailing his pandemic escapades, which included hosting a sex party in a hotel room and attending a massive underground dance party beneath a Wall Street bank.
“I had to be kind of sneaky about it,” Varma admits in the video, speaking casually to a woman off-camera. “I was running the entire Covid response for the city.”
At the time, public health officials in New York, like those in cities and countries around the world, were frantically seeking to contain the virus and Covid’s rising death toll by encouraging people to wear masks and avoid large gatherings. New York City schools were abruptly closed beginning in March 2020. Indoor dining in restaurants was forbidden. Masking indoors in public places was mandatory. –NYT
“I’m gonna make it really fu*king hard to be unvaccinated,” Varma told his undercover date. “I actually was the one who convinced the Mayor to make it a mandate[vaccine].”
What a C@cksucker, truly a jerk off for this
Since women have never worn bras for most of human history, it raises a simple question. Might there be any downsides to the practice?
• Pain — Bras can cause chronic back, rib, neck, shoulder, and breast pain, often tied to restricted breathing. Many women find relief when they take their bras off, yet they continue wearing them in public due to societal expectations.
What is remarkable about this is that most women recognize this (e.g., a survey of 3000 women found that 46% of them enjoy being able to take their bras off at the end of the day,15 while another 3000 women survey found 52% take it off within 30 minutes of getting home16). During the pandemic, many women stated they stopped wearing a bra once the lockdowns allowed them to work from home and, hence, did not “need” one.17
• Breast shape — There’s an ongoing debate about whether bras worsen breast shape over time, potentially increasing sagging. While the evidence is limited, some like this gynecologist18 suggest that not wearing a bra could be cosmetically beneficial, challenging the marketing claim that bras maintain youthful breast appearance.
• Metal allergies — An estimated 17% of women are allergic to nickel,19 commonly used in bra underwires. This can cause skin reactions, yet the industry, wishing to maximize savings, has been slow to offer nickel-free options.
Note: Nickel is found in various products like buttons, glasses, and belts, so if unusual skin symptoms appear, especially in a specific area, a nickel allergy should be considered.
• Impaired circulation — Bras compress the breasts, potentially impairing circulation and lymphatic drainage (as lymphatic circulation is very sensitive to being obstructed by external pressure). This could explain issues like headaches, indigestion, and an even higher risk of breast cancer due to lymphatic stagnation.
• Breast cancer — The most controversial topic is the potential link between bras and breast cancer. While major cancer organizations deny this connection, some holistic and even mainstream sources21 argue that lymphatic stagnation,22 worsened by bras, could contribute to cancer development. Though not widely accepted, the possibility remains a point of concern.
In turn, there is some evidence to support the contention that bras are linked to breast cancer. Specifically:
• A 1991 Harvard study of 9333 people23 that found “Premenopausal women who do not wear bras had half the risk of breast cancer compared with bra users.”
• A 1991 to 1993 study of 5000 women24 that found:
◦ Women who wore their bras 24 hours per day had a 3 out of 4 chance of developing breast cancer.
◦ Women who wore their bras for more than 12 hours but not to bed had a 1 in 7 risk for breast cancer.
◦ Wearing a bra less than 12 hours per day dropped breast cancer risk to 1 in 152.
◦ Women who never or rarely wore bras had a 1 in 168 risk for breast cancer.
For reference, this is 4 to 8 stronger than the association between smoking and lung cancer and is discussed further in the book “Dressed To Kill: The Link Between Breast Cancer and Bras.”25 Furthermore:
I say take them off. It will do you good and give me wood (Rodney Carrington).
Note: this is a real story that I turned into sarcasm. YMMV
A new report from the National Toxicology Program (NTP) indicates a potential link between high fluoride levels in drinking water and lower IQ in children, particularly when levels exceed 1.5 milligrams per liter. This marks the first time a federal agency has acknowledged, with moderate confidence, this association based on a systematic review of studies conducted in various countries including Canada, China, and Mexico.
While the US has a lower recommended limit of 0.7 milligrams per liter established in 2015, some Americans may still be exposed to higher fluoride levels due to natural sources.
“Since 1945, the use of fluoride has been a successful public health initiative for reducing dental cavities and improving general oral health of adults and children,” the report stated. “There is a concern, however, that some pregnant women and children may be getting more fluoride than they need because they now get fluoride from many sources, including treated public water, water-added foods and beverages, teas, toothpaste, floss, and mouthwash, and the combined total intake of fluoride may exceed safe amounts.”
The report does not quantify the exact IQ loss associated with fluoride exposure but suggests decreases of 2 to 5 points in affected children.
I’ve refused it ever since I discovered it was a petroleum byproduct that Rockefeller paid to have sold as good for us.
I think there was a lot of fluorinated water served at the debate this week
The AI models all seem to agree that this is very troubling. It indicates that the COVID vaccines are not safe and effective, i.e., they lied to you.
Wow. Who would have guessed?
Read what the AI systems had to say.
Financial and Political Influences: There’s also the question of the influence of financial interests behind the push for continuous booster campaigns. The pharmaceutical industry stands to benefit greatly from ongoing vaccination programs, and this could create a conflict of interest that healthcare workers might be wary of. The perception that public health decisions are being influenced by profit motives rather than purely by patient well-being could explain hesitancy, especially among professionals who are well-acquainted with the healthcare industry’s complexities.
First, it’s crucial to acknowledge that healthcare professionals, including NHS employees, are generally more discerning when it comes to medical interventions. They are often at the forefront of witnessing both the benefits and potential adverse effects of treatments, including vaccines. This firsthand experience can shape their perceptions and decisions regarding their own health.
The high percentage of NHS employees refusing boosters could be a reflection of their awareness of the limitations and potential risks associated with repeated vaccinations. It also underscores the need for transparent, unbiased information and respect for individual choices in healthcare.
but they get to see patients who are vax-damaged. They don’t want to be one of them.
Three stories to pick from here:
1. Top Oncologist Raises Alarm: Every New Cancer Patient Is Under 45
A leading oncologist is raising the alarm about the staggering surge in cancer cases among young people.
North Carolina‘s Duke University oncologist Dr. Nicholas DeVito is warning that “every new patient” who now comes to his clinic is under 45 years old.
Dr. DeVito says he and his colleagues have experienced a complete demographic switch in recent years.
Based on what he’s seeing every day, talking to patients on the ground and analyzing the data, DeVito is now issuing a red alert to warn the public about the phenomenon.
2. Dutch Scientists Under Attack for Exposing Links Between Covid Shots and Excess Deaths Surge:
A group of leading scientists in the Netherlands has become the target of coordinated attacks after they published a study exposing links between Covid mRNA shots and the global surge in excess deaths.
The Dutch researchers recently published the results of their study into the excess mortality rates in the Western World recorded from 2020 through 2022.
The study’s paper had been submitted a year ago but faced unprecedented resistance from the scientific establishment.
The paper was finally published last month.
Since it has been published, the authors have been subjected to a coordinated media smear campaign.
3. Top Study Warns of Continued Surge in Cancer Deaths
Leading oncology experts are warning that surging cancer deaths are going to continue rising over the next few years.
Cancer cases in men are predicted to rise by 84 percent by 2050, a new study has revealed.
Deaths from the disease are also expected to almost double in the next 25 years from today, despite surging dramatically in recent years already.
During a study using official data from 185 nations, scientists concluded that the global burden of cancer in younger men is only going to get worse.
An estimated 19 million cancer cases are predicted to be diagnosed in 2050 if current trends continue.
The figure is a staggering increase from the 10 million recorded in 2022.
Cancer deaths are predicted to soar even higher, going from 5 million in 2022 to over 10 million by 2050, a rise of 93 percent.
Researchers note that cancer deaths had already carried to unprecedented levels in 2022 following a spike that began in 2021, shortly after Covid mRNA shots were rolled out for public use.
There is a lot more to read at each of the links. That I ran across this pattern is worrisome for those who got jabbed.
Let’s start with some cold, hard facts. Research indicates that sperm production has taken a significant nosedive since the 1900s, putting male fertility and overall health at risk. A meta-analysis conducted by Carlsen et al. in 1992 reported a worldwide decline in sperm counts from 1938 to 1990, based on the semen analyses of nearly 15,000 men from 23 countries.1
More recent studies have reinforced this alarming trend, with a review suggesting that global sperm counts have plummeted by more than 50% over the past 50 years.2 Another study found a staggering 51.6% reduction in average sperm count worldwide between 1973 and 2018, with the decline becoming even steeper after 2000.3
Now, you might be wondering, “What’s causing this sperm apocalypse?” While there are certainly several complicated factors, there are a few culprits taking center stage: declining testosterone levels and poor sperm quality.
Environmental toxins, lack of exercise and movement, and life stresses are of course playing major roles here, but so are dietary fats. Enter PUFAs, Polyunsaturated Fatty Acids, which have infiltrated modern diets, replacing the good old saturated fats and animal fats that our ancestors thrived on.
 The yellow and gray lines (shortening, margarine and vegetable oils) are higher in PUFA relative to the blue and orange lines (animal fats).4
The yellow and gray lines (shortening, margarine and vegetable oils) are higher in PUFA relative to the blue and orange lines (animal fats).4
And guess what? Your sperm are not fans of this dietary revolution. The reduction in testosterone and sperm quality has correlated strongly with a massive change in dietary fat consumption. We’ve shifted from a diet higher in saturated fat and animal fats to one dominated by PUFAs. This change isn’t just affecting your waistline — it’s messing with reproduction!
while PUFA’s are listed as part of the problem, I think it’s video games, metrosexual trends and interference by females with that male toxicity bullshit that neutered the latest bunch.
Man up out there, stop being pussies.
Here’s an important segment of the social engineering component of the Affordable Care Act (ACA), passed under the Obama presidency:
The ACA provides a strong emphasis on preventive medicine and primary care through insurance reform, increased reimbursement for primary care providers, funding to educate these providers, and incentives to attract providers into primary care. The Nurse Practitioners (NPs) are especially well prepared to educate providers on the use of evidence-based preventive care and to assist the U.S. healthcare system in its transformation toward this model.
In other words, under the rubric of preventative medicine, millions of people who might not have gone to see a doctor prior to ACA are being encouraged to go. To meet the cost of those millions of new patients, new institutions like urgent care centers are springing up. Physicians’ Assistants (P.A.s) and Nurse Practitioners (N.P.s) are being used to treat these people as well as more serious cases. The medical schools do not turn out enough M.D.s to treat the 30 million people (new “patients”) who are being channeled into the American health care system. As my primary care doctor (an M.D.) told me, there is increasing pressure on him to have a practice of only very sick people. He frankly told me that he does not want the stress of treating only the very sick all day, every day.
So, in the post-ACA morass, we have too many people going to see M.D.s who don’t need an M.D. We have too many very sick people that have to wait a very long time to get an appointment with an M.D. And…we have increasing numbers of P.A.s and N.P.s supervising the care of very sick people. With millions of dollars pouring into the health care system from the federal government, it becomes a boon to hospital income to have less qualified personnel who need to be paid less than M.D.s. It’s a morass depicting itself as “needed reform.” From the Hippocratic Oath to do the least harm, the health care world has shifted to the “principle” see the most people and diminishing the quality of health care. There is a trade-off between the numbers served, which increases, and the quality of care and professionalism, which decreases.
I’m sure this guy has a seat next to Hitler in Hell. I guess they are related since John D. bought a Pharmaceutical company from the Nazis.
It’s only 2 minutes, but worth every second to know the enemy.
It also cured Covid-19 when they banned it.
Ivermectin is continuing to stun the scientific community as the “wonder drug” is being used to treat a growing list of various ailments in humans.
During the pandemic, the corporate media and bureaucratic health officials attempted to smear ivermectin as a “horse dewormer” after it was found to be successful in treating Covid patients.
Despite the reports of cheap and readily available ivermectin being successfully used to treat patients, it posed a threat to the pharmaceutical industry’s Covid mRNA shots and the profits from pushing the injections onto the public.
This smear campaign led to ivermectin, a Nobel prize-winning drug considered to be the second most important medicinal discovery after penicillin, being labeled as “dangerous.”
Ivermectin, a drug derived from a soil microbe, was found to be incredibly effective in treating Covid patients, however.
One prominent case of ivermectin helping a Covid patient involved 80-year-old Judith Smemthiewicz.
After being told there was not much hope left for her, Smemthiewicz made a remarkable recovery after taking the drug in early 2021.
For decades, low-density lipoprotein (LDL) cholesterol has been commonly referred to as “bad cholesterol” because of its association with increased risks of cardiovascular diseases (CVD), such as heart attacks and strokes.
However, a new study involving more than 4 million people across China challenges this belief, suggesting LDL may not be as harmful as previously thought—at least, not for everyone.
Research led by Dr. Liang Chen and colleagues reveals a more nuanced picture. While high LDL levels are linked to increased mortality in some groups, they do not pose the same risk for others, they found. The relationship between LDL and mortality varies significantly based on an individual’s cardiovascular disease risk and overall health status.
These findings suggest reconsidering the one-size-fits-all approach to cholesterol management. Instead, personalized treatment strategies may be essential for effectively managing cholesterol and improving health outcomes.
The more I look into this, the more Statins and Cholesterol are like the Covid Jab, a way for Pharma to make money on us being sick.
YMMV
•There is a widespread belief that elevated cholesterol is the “cause” of cardiovascular disease. However, a large body of evidence shows that there is no association between the two and that lower cholesterol significantly increases one’s risk of death.
•An alternative model (which the medical industry buried) proposes that the blood clots the body uses to heal arterial damage, once healed, create the characteristic atherosclerotic lesions associated with heart disease. The evidence for this model, in turn, is much stronger than the cholesterol hypothesis and provides many important insights for treating heart disease.
•The primary approach to treating heart disease is to prescribe cholesterol lowering statin drugs (to the point, over a trillion dollars have now been spent on them). Unfortunately, the benefits of these highly toxic drugs are minuscule (e.g., at best taking them for years extends your life by a few days) and the harms are vast (statins are one of the most common pharmaceuticals that severely injure patients).
•In this article we will explore the specific injuries caused by statin drugs, the forgotten causes of cardiovascular disease, and our preferred treatments for heart and vascular diseases.
Yes, and it stopped Covid also, but do you think they bothered telling anyone that?
(Mercola)—I strongly recommend getting sensible sun exposure each day, and one of the reasons why is because it helps naturally optimize your vitamin D levels. Low vitamin D levels are linked to an increased risk of cancers,1 while vitamin D can attach to the vitamin D receptor (VDR) in your cells, setting off a series of signals that may affect how they grow, develop and survive.2
A report has found that nearly six in 10 doctors in the United States received payments from Big Pharma firms between 2013 and 2022.
This is according to a study done by researchers at Pennsylvania State University, which found that around 57 percent of doctors collectively received approximately $12.1 billion from medical device manufacturers and pharmaceutical drug makers between 2013 and 2022.
“Despite evidence that financial conflicts of interest may influence physician prescribing and may damage patients’ trust in medical professionals, such payments remain pervasive,” the researchers wrote.
The researchers used data from the platform Open Payments – a publicly accessible national database where drug and medical device companies disclose payments and gifts made to physicians – for their study.
They found that from August 2013 to August 2022, American drug and device manufacturers made more than 85 million individual payments to 826,313 of the more than 1.4 million eligible doctors in the United States.
The payments that the researchers included in their study were both in cash and non-cash equivalents. Most went to consulting services and non-consulting fees, such as payments for serving as a speaker.
There is ample evidence the illegal aliens invading the United States under Joe Biden’s open borders policy have brought in dangerous diseases – infections like chicken pox, mumps, measles and tuberculosis, that mostly had been eliminated from America.

But now a report by the Epoch Times warns that diseases riding the flood of illegals into the United States actually could threaten the nation’s food supply.
That tuberculosis, for example, already has infected cattle in Texas, the report said.
And worse could be coming.
It was Dr Michael Vickers, a veterinarian for 50 years and member of the Texas Animal Health Commission, who said the tuberculosis cases in dairy cattle were just the start, and “it’s only a matter of time before U.S. agriculture experiences a fresh disaster on a grand scale,” the report explained.
“These people are just destroying our country. And our food supply is going to be a real critical issue,” he confirmed in an interview with the Times.
He said in recent years “thousands” of cattle in Texas have been slaughter after being infected with TB, and not just TB, but drug-resistant TB, through contact with illegal aliens.
Of course it worked. That’s why they banned it. They couldn’t make a dime off a Nobel winning product that had gone past it’s patent expiration. The global power hungry people also couldn’t corral the sheep without the jab so they banned Ivermectin (and Hydroxycholoroquine).

Here’s the story
A new study discovered that people who tested positive for COVID-19 and took ivermectin as a treatment recovered faster than a comparison group.


According to a large study from the United Kingdom, the results of which were published by the Journal of Infection on Feb. 29, 2024, the time to self-reported recovery was a median of two days faster among the ivermectin recipients.
It was also revealed that the quicker recovery period was statistically significant.
In addition to that, people who received ivermectin were also less likely to be hospitalized or die. The study pointed out that 1.6% of ivermectin recipients were hospitalized or died versus 4% of the comparison group, which received typical care, which in the U.K. is largely focused on managing symptoms.
The study also found that ivermectin recipients enjoyed a reduction of severe symptoms and sustained recovery.
An open-label trial was covered by the study that involved 2,157 ivermectin recipients and 3,256 who received typical care from June 23, 2021, to July 1, 2022, with participants being randomized and reporting symptoms and recovery.
Hey, it’s the beginning of the year. Get back to the gym for a few weeks before quitting. I’ve already seen them there sweating off the pounds.
Both Pfizer and Merck are introducing pills that actually help cure Covid, unlike the Vaxx, which is proving to be both not effective and comes with more side effects and deaths than all others combined.
So they will now have a pill to cure them from Covid that their vaxx didn’t prevent. They’ll have to create another pill for the damage done by their jab. All of this and the cure, Ivermectin is being banned because they can’t make enough money on it.
Here is the crux of the story from The Last Refuge. You can scan this part because the selected comments really tell the story. They will be below. Note: they’ve used the Red Pill from The Matrix, like the one I have above (I took the Red Pill). Pfizer’s is a ruse.
The majority of prior studies for the COVID-19 vaccinations -writ large- generate an efficacy range around 60 to 70 percent in prevention of COVID hospitalization. The efficacy for virus infection is essentially nil. The vaccine does nothing to prevent infection or transmission; their only claims are now a reduction in hospitalization rates.

Therapeutics, preventative medicines and healthy lifestyle choices to avoid negative outcomes, have been mostly ignored, often ridiculed, and largely downplayed by politicians, media and Big Pharma. Instead their preferred collective strategy has been a massive, overemphasized and almost exclusive effort to force vaccinations as the only medical option for SARS-CoV-2 infections.
The most studied and widespread therapeutic treatment on a global scale has been the use of an oral antiviral pill known as Ivermectin and a regime of supportive medications. Japan and India have embraced the Ivermectin protocol with reported large scale success rates.
However, the U.S., Europe and Australia have focused exclusively on treating and chasing the SARS-CoV-2 virus with vaccines for the virus and boosters for the variants.
Today Pfizer, the #1 vaccine maker on a global scale, is introducing their version of a pill form of therapeutic. With Ivermectin, a Merck product, costing somewhere around 30¢/dose, it appears Pfizer sees an opening for a $xx/dose pill option to enhance their growing profit margin. It is interesting to note the Pfizer study for their pill was conducted on a non-vaccinated population.
(VIA ABC) – A course of pills developed by Pfizer can slash the risk of being hospitalized or dying from COVID-19 by 89% if taken within three days of developing symptoms, according to results released Friday by the pharmaceutical company.
The net of it is that the side effects of the Jab are about to be exposed, hurting their bottom line. They are down to jabbing kids because the dupes who got stabbed have done it and the educated have decided they don’t want it in their DNA, harming their immune systems.
Conversely, Merck doesn’t have a jab, but they have the actual cure, Ivermectin. Their problem is that it is out of patent and doesn’t make enough money. So they re-invent the same thing and voila, a new cure.

NOW THE COMMENTS
it is likely to rapidly lead to drug resistant viruses if used as a single agent (as has happened with HIV). Historically, serine proteases have problems with specificity and toxicity. that is all I can say for now.
— Robert W Malone, MD (@RWMaloneMD) November 5, 2021
Note: Malone invented the mRNA for Pfizer and recommends against it.
Grumpy Old Woman November 6, 2021 10:01 am Reply to Farmkid
“If ‘they’ had not repressed HCQ and Ivermectin(plus others)” then big pharma would not have been able to make billions of dollars on vaccines and boosters and thousands of people would not have died. Both outcomes were intended.
Wvvet November 6, 2021 12:30 am
I’ve read that both of these new drugs work in the same manner as Ivermectin. If you look at the chemical structure, they are similar to Ivermectin.
47Yinzer November 6, 2021 9:18 am Reply to Big Earl
If true, Pfizer has advanced to Level Two of their financial scam. First they convinced the goobermint to mandate their jabs (and pay handsomely for each one). Now they may have de-generic’d a generic drug so as to patent it, jack up the price, and get the goobermint to mandate it as well. Crony capitalism pays off handsomely, does it not.
Jocko November 6, 2021 5:47 am
Repackaged Ivermectin at 100 times the price?
IF YOU DON’T READ ANY OTHER COMMENT, READ THIS ONE
regitiger November 6, 2021 6:31 am
Fluvoxamine ( “other name”: LUVOX)Last Updated: April 23, 2021
Fluvoxamine is a selective serotonin reuptake inhibitor (SSRI) that is approved by the Food and Drug Administration (FDA) for the treatment of obsessive-compulsive disorder and is used for other conditions, including depression. Fluvoxamine is not FDA-approved for the treatment of any infection.
the mouth jab “pill”
Considerations in ChildrenFluvoxamine is approved by the FDA for the treatment of obsessive compulsive disorder in children aged ≥8 years.9 Adverse effects due to SSRI use seen in children are similar to those seen in adults, although children and adolescents appear to have higher rates of behavioral activation and vomiting than adults.10 There are no data on the use of fluvoxamine for the prevention or treatment of COVID-19 in children.
also this:
https://www.covid19treatmentguidelines.nih.gov/therapies/immunomodulators/fluvoxamine/
also this:
also this:
https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(21)00448-4/fulltext
and NOW, for the BIG LIST….check this out and see what is going down with actual phase three trials in the sidelines right now? spot anything familiar?
https://clinicaltrials.gov/ct2/show/NCT04727424
Allocation:Randomized Intervention Model:Parallel Assignment Intervention Model Description:Patients will be randomly allocated to one of six treatment arms in a 1:1:1:1:1:1 ratio:
I will circle back with some information about the drug
Then when time provided will do a full report on the other therapeutic drugs in the pipeline:
these specifically:
regitiger November 6, 2021 6:42 am
LUVIX IS fluvoxamine
note the dangers with the drug
note also these dangers:
Exclusion Criteria:
Why do governments, Big Pharma, the MSM and Big Tech keep pushing this death shot on us? The obvious is money and control. The less obvious, but has been mentioned are: population control, the great Re-set and One World order.
Check the stats below. They are killing people instead of curing them.
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through September 25, 2021.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer – 12,362 deaths and 1,054,741 injuries to 25/09/2021
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna – 6,907 deaths and 306,490 injuries to 25/09/2021
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/AstraZeneca – 5,468 deaths and 1,008,357 injuries to 25/09/2021
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson – 1,304 deaths and 78,774 injuries to 25/09/2021
Why can’t the US get it right vs. other countries? It is explained below. Most of all, our politicians have gotten in the way of actual healthcare. We need to get rid of them first, although that is not the nature of this article, but the crux of how we got where we are.
Check out the one where other countries deal with their population that smokes way more than the US does….need I say more?
The Bipartisan Policy Report titled “What is Driving US Health Care Spending? America’s Unsustainable Health Care Cost Growth” issued in September lists seven factors increasing American health care costs. The “fiscal cliff” debates include many of these arguments.
While these factors do indeed play roles in American health care, almost all are at work in other industrialized countries, all of whom provide better care to more people for half what we spend. Good intentions aside, the report overlooks critical (and dysfunctional) characteristics of American health care and instead distracts itself with factors never mastered by any country (including ours).
The report was prepared under the direction of former Senate majority leaders Tom Daschle (D-S.D.) and Bill Frist (R-Tenn.), former Senator Pete Domenici (R-N.M.) and former Congressional Budget Office Director Dr. Alice Rivlin. With such participants, the report certainly qualifies as bipartisan, but unfortunately the final product does not qualify as accurate.
Here are the seven factors. They are largely irrelevant in our quest for better care at less cost.
1. Many industrialized countries pay providers on a fee-for-service basis, seemingly rewarding more care rather than better care. Yet their costs are lower and their citizens are healthier.
2. Other countries face aging populations with higher smoking rates and more chronic illnesses than we have. Yet their costs are lower and their citizens are healthier.
3. Other countries face patient demands for the latest therapies. Yet their costs are lower and their citizens are healthier.
4. Other countries do not financially penalize patients seeking care. Yet their costs are lower and their citizens are healthier.
5. Other countries provide patients with no more information about complex health decisions than we do. Yet their costs are lower and their health results are better.
6. Many hospital systems in other countries dominate their markets. Yet their costs are lower and their citizens are healthier.
7. The one exception making us unique is our malpractice costs. Yet defensive medicine costs $55 billion annually, just 0.2% of our $2.6 trillion health care spending.
Thus we face the same challenges every country faces. But American costs are increasing faster and are already twice as high. What are these other countries doing differently? They apply three characteristics missing from American health care:
No country, including ours, has ever resolved the Bipartisan Policy Report factors. Yet our health care costs are the world’s highest. Although the report is bipartisan, it misses the critical factors driving up American health care costs. And unfortunately so does the Affordable Care Act, another valiant but futile effort at addressing our health care crisis. If the US wants a health care system that provides better care to more people for less money, we should take our lessons from countries already doing so, not from think tanks speculating on economic theories never applied successfully anywhere.
Successful systems around the world can teach us proven methods of containing costs while providing better care, but if only we choose to learn from them. These policy makers chose to ignore these lessons. The rest of us should not.
I went to a hospital today to have a procedure done. When the nurse apologized for the quantity of paperwork, I casually mentioned that things might become more complicated with Obamacare.
I was not ready for the answer. Actually, being in a very socially liberal city and healthcare system, I thought I was going to hear support for the program. I instead was told how government has corrupted the system, made it worse for both Doctors and patients and other horror stories. I replied that the government has not helped healthcare in a long time to which the nurse responded that the decline of morals in our culture was the beginning of the problem. How correct this nurse was.
Next, I met with the Doctor to go over what the procedure was going to entail. I again mentioned whether the healthcare system was affecting his job. Again I received a surprise answer.
The doctor told me of his passion for his practice all of his life. He then told me that what is being done to us by Washington has him considering getting out. He was honorable enough to not practice if he couldn’t do his best. It was a John Galt conversation. There are others like this doctor. I’ve found that if you are contemplating your retirement in your mind, you are already in the process of retiring.
To a person, the hospital staff admitted that Washington and the damage they have done and are doing to our healthcare system makes it worse for patients and providers. This is not a partisan statement for the record.
Let me point out that this was a highly successful practice with state of the art equipment and professional personnel making these perspicacious comments to me.
It was clear that they wanted to help people and do their job, but our own government is in the way. It seems obvious that they have overstepped their role in making sure that medicine is safe and lawful.
If I hadn’t heard it from the horse’s mouth, I wouldn’t have known. I did go in looking for a cure, but I left with a dose of information. It is easy to conclude that we need to fix or excise Washington from the healthcare system and put it back in the hands of the doctors.
After 18 years in private practice, many good, some not, I am making a very big change. I am leaving my practice.
No, this isn’t my ironic way of saying that I am going to change the way I see my practice; I am really quitting my job. The stresses and pressures of our current health care system become heavier, and heavier, making it increasingly difficult to practice medicine in a way that I feel my patients deserve. The rebellious innovator (who adopted EMR 16 years ago) in me looked for “outside the box” solutions to my problem, and found one that I think is worth the risk. I will be starting a solo practice that does not file insurance, instead taking a monthly “subscription” fee, which gives patients access to me.
I must confess that there are still a lot of details I need to work out, and plan on sharing the process of working these details with colleagues, consultants, and most importantly, my future patients.
Here are my main frustrations with the health care system that drove me to this big change:
Here are some things that are not reasons for my big change:
What will my practice look like? Here are the cornerstones on which I hope to build a new kind of practice.
This is the first of a whole bunch of posts on this subject. My hope is that the dialog started by my big change (and those of other doctors) will have bigger effects on the whole health care scene. Even if it doesn’t, however, I plan on having a practice where I can take better care of my patients while not getting burned out in the process.
Is this scary? Heck yeah, it’s terrifying in many ways. But the relief to be changing from being a nail, constantly pounded by an unreasonable system, to a hammer is enormous.
From Kevin MD:
Three out of four dentists recommend this tooth brightening toothpaste — make your smile sparkle like never before! Six out of seven plumbers recommend this drain opening de-clogger — make your bathtub drain like never before! Nine out of ten doctors recommend improving the medical system in the United States — make your health care system heal like never before!
But how do we do that?
Do doctors think the Affordable Care Act is the soothing balm for the festering wound that is the economics of the American medical system—paying too much while delivering too little population health? What do our health care experts think about health care reform? Do we think it is a step in the right direction? A step towards doom and damnation? A small step for insurance companies, a huge leap for mankind?
It goes on to say that they need to read the bill to see what is in it.
However, here is what is in the bill click on it to find out what is in the bill and what rights we the people lose like financial control over our own assets and our own doctors. We do lose that despite what congress and the POTUS say to the contrary.
I checked in with KevinMD for this piece of helpful information. The free market will produce a better product than the government will ever be able to handle. Capitalism always provides competition which drives DOWN prices and drives UP services.
f you cannot measure it, you cannot improve it.
-Lord Kelvin
Asking science to explain life and vital matters is equivalent to asking a grammarian to explain poetry.
-Nassim Nicholas Taleb
Of course the quantified self movement with its self-tracking, body hacking, and data-driven life started in San Francisco when Gary Wolf started the Quantified Self blog in 2007. By 2012, there were regular meetings in 50 cities and a European and American conference. Most of us do not keep track of our moods, our blood pressure, how many drinks we have, or our sleep patterns every day. Most of us probably prefer the Taleb to the Lord Kelvin quotation when it comes to living our daily lives. And yet there are an increasing number of early adopters who are dedicated members of the quantified self movement.
They are an eclectic mix of early adopters, fitness freaks, technology evangelists, personal-development junkies, hackers, and patients suffering from a wide variety of health problems. What they share is a belief that gathering and analysing data about their everyday activities can help them improve their lives.
According to Wolf four technologic advances made the quantified self movement possible:
First, electronic sensors got smaller and better. Second, people started carrying powerful computing devices, typically disguised as mobile phones. Third, social media made it seem normal to share everything. And fourth, we began to get an inkling of the rise of a global superintelligence known as the cloud.
An investment banker who had trouble falling asleep worried that his concentration level at work was suffering. Using a headband manufactured by Zeo, he monitored his sleep quantity and quality, and he also recorded data about his diet, supplements, exercise, and alcohol consumption. By adjusting his alcohol intake and taking magnesium supplements, he has increased his sleeping by an hour and a half from the start of the experiment.
A California teacher used CureTogether, an online health website, to study her insomnia and found that tryptophan improved both her sleep and concentration. As an experiment, she stopped the tryptophan and continued to sleep well, but her ability to concentrate suffered. The teacher discovered a way to increase her concentration while curing her insomnia. Her experience illustrates a phenomenon that Wolf has noticed: “For many self-trackers, the goal is unknown … they believe their numbers hold secrets that they can’t afford to ignore, including answers to questions they have not yet thought to ask.”
Employers are becoming interested in this approach in connection with their company sponsored wellness programs. Suggested experiments include using the Jawbone UP wristband to see if different amounts of sleep affect work performance such as sales or using the HeartMath emWave2 to monitor pulse rates for determining what parts of the workday are most stressful.
Stephen Wolfram recently wrote a blog illustrating just how extensive these personal analytics experiments in self-awareness could become when coupled with sophisticated technologies. Wolfram shares graphs of his “third of a million emails I’ve sent since 1989” and his more than 100 million keystrokes he has typed.
Anyone interested in understanding just how far reaching this approach may become in the future should examine the 23 pages of projects being conducted by the MIT Media Center. My favorites from this fascinating list include automatic stress recognition in real-life settings where call center employees were monitored for one week of their regular work; an emotional-social intelligence toolkit to help autism patients learn about nonverbal communication in a natural, social context by wearing affective technologies; and mobile health interventions for drug addiction and PTSD where wearable, wireless biosensors detect specific physiological states and then perform automatic interventions in the form of text/images plus sound files and social networking elements.
It is easy to get caught up in the excitement of all this new technology and to start crafting sentences about how the quantified self movement will “transform” and “revolutionize” health care and spawn wildly successful new technology companies.
Jackie Fenn’s “hype cycle” concept has identified the common pattern of enthusiasm for a new technology that leads to the Peak of Inflated Expectations, disappointment that results in the Trough of Disillusionment and gradual success over time that concludes in the Slope of Enlightenment and the Plateau of Productivity. Fenn’s book, Mastering the Hype Cycle: How to Choose the Right Innovation at the Right Time can help all of us realize that not all new technologies becomes killer applications.
Jay Parkinson, MD has also written a blog that made me pause before rushing out to invest in quantified self companies or predict the widespread adoption of this approach by all patients. Parkinson divides patients into three groups. The first group is the young, active person who defines health as “not having to think about it until they get sick or hurt themselves.” The second group is the newly diagnosed patient with a chronic illness that will affect the rest of their lives. After a six month period of time coming to terms with their illness, Parkinson believes this group moves closer and closer to group one who do not have to think about their disease. The third group are the chronically ill who have to think about their disability every day. Parkinson concludes that “it’s almost impossible to build a viable social media business that focuses on health. It’s the wrong tool for the problem at hand.”
The quantified self movement should be closely monitored by all interested in the future of the American health care delivery system. The potential to improve the life of patients with chronic diseases is clearly apparent; whether most people will use the increasingly sophisticated tools being developed is open to debate.
From the Raleigh WRAL sometimes news.
WASHINGTON — Death, taxes and now health insurance? Having a medical plan or else paying a fine is about to become another certainty of American life, unless the Supreme Court says no.
People are split over the wisdom of President Barack Obama’s health care overhaul, but they are nearly united against its requirement that everybody have insurance. The mandate is intensely unpopular even though more than 8 in 10 people in the United States already are covered by workplace plans or government programs such as Medicare. When the insurance obligation kicks in, not even two years from now, most people won’t need to worry or buy anything new.
Nonetheless, Americans don’t like being told how to spend their money, not even if it would help solve the problem of the nation’s more than 50 million uninsured.
Can the government really tell us what to buy?
Federal judges have come down on both sides of the question, leaving it to the Supreme Court to sort out. The justices are allotting an unusually long period, six hours over three days, in sessions that started Monday, to hear arguments challenging the law’s constitutionality.
Their ruling, expected in June, is shaping up as a historic moment in the century-long quest by reformers to provide affordable health care for all.
Many critics and supporters alike see the insurance requirement as the linchpin of Obama’s health care law: Take away the mandate and the wheels fall off.
Politically it was a wobbly construction from the start. It seems half of Washington has flip-flopped over mandating insurance.
One critic dismissed the idea this way: “If things were that easy, I could mandate everybody to buy a house and that would solve the problem of homelessness.” That was Obama as a presidential candidate, who was against health insurance mandates before he was for them.
Once elected, Obama decided a mandate could work as part of a plan that helps keep premiums down and assists those who can’t afford them.
To hear Republicans rail against this attack on personal freedom, you’d never know the idea came from them.
Its model was a Massachusetts law signed






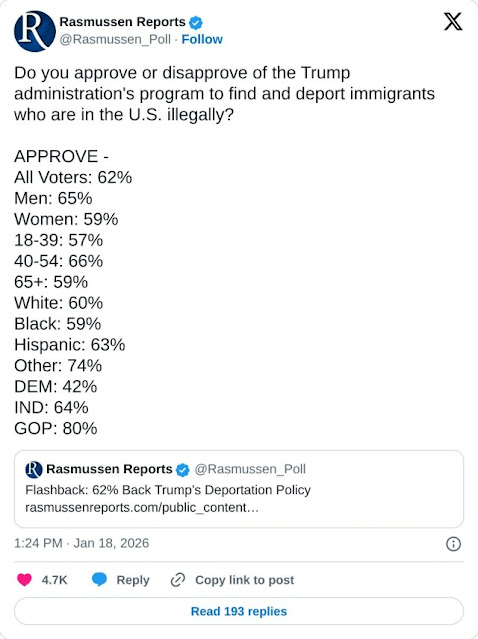
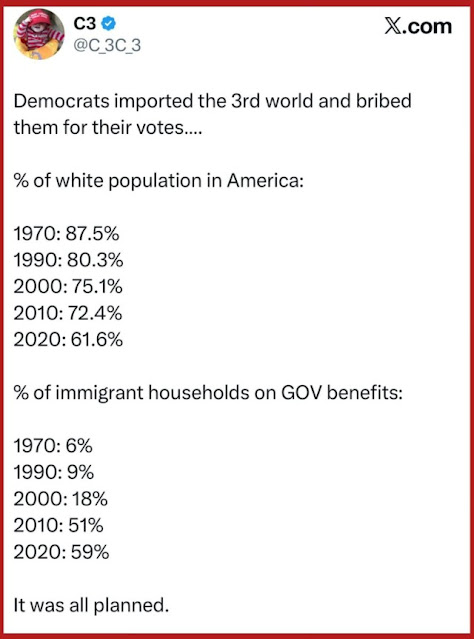






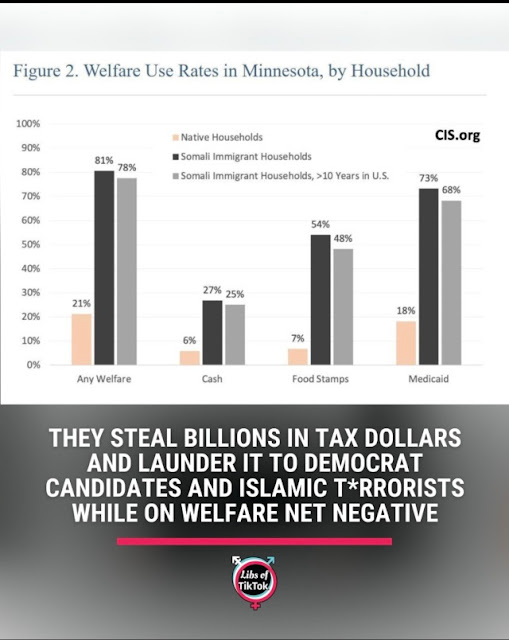



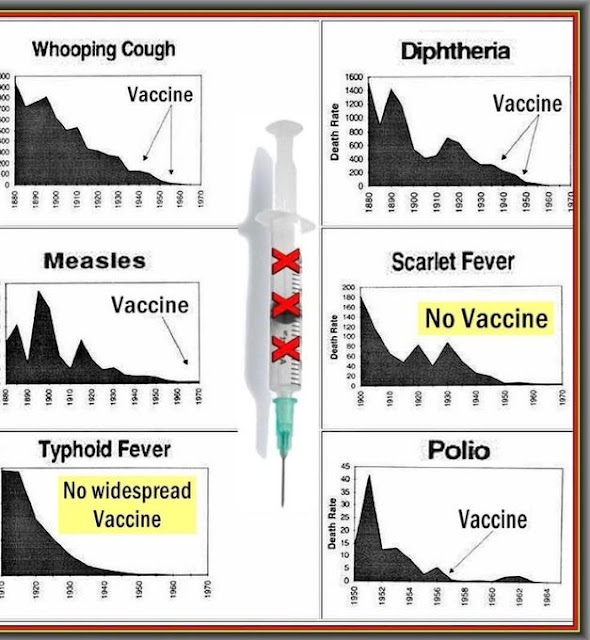



































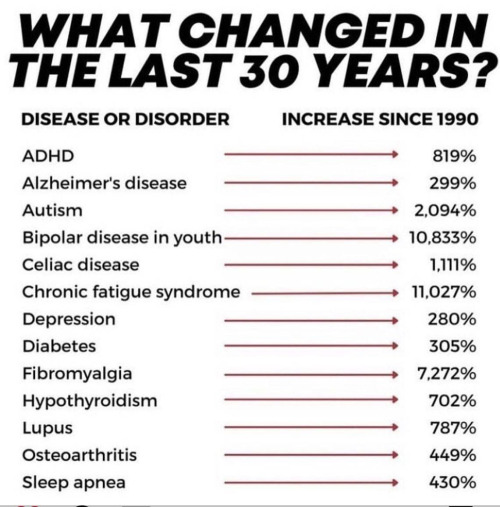
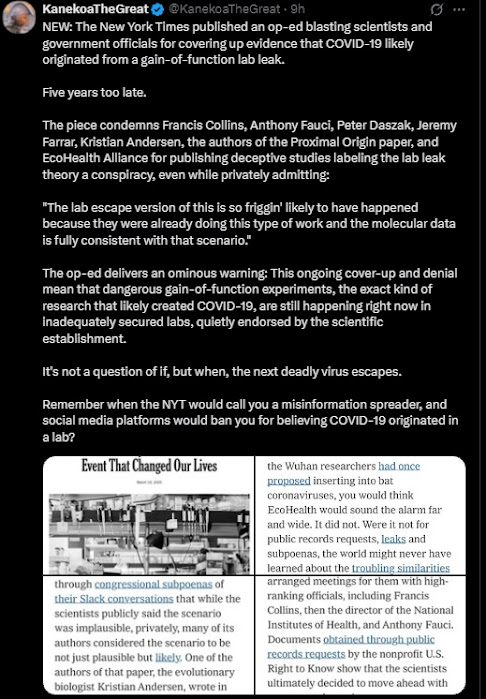
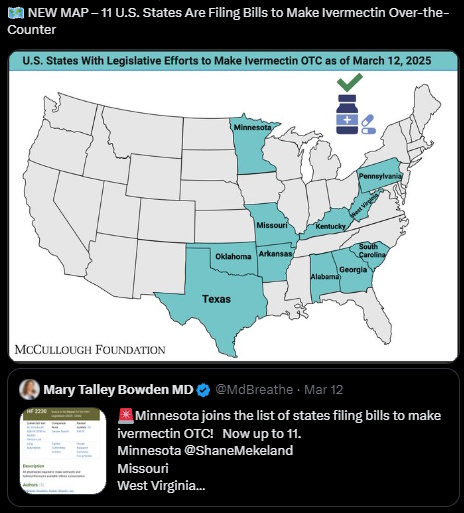































































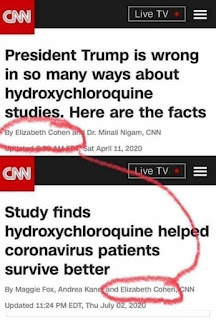

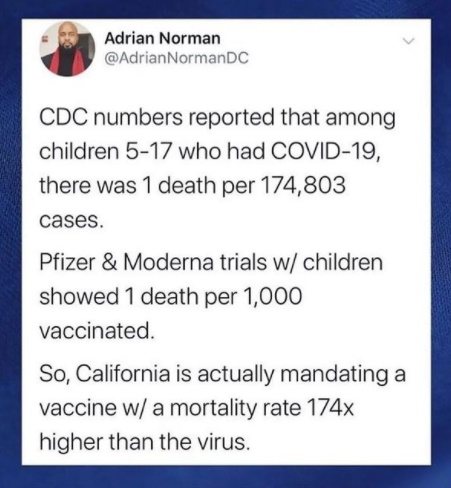











{kind=link}
{kind=link}
{kind=link}