

Here are the 10 biggest falsehoods—known for years to be false, not recently learned or proven to be so—promoted by America’s public health leaders, elected and unelected officials, and now-discredited academics:
1. SARS-CoV-2 coronavirus has a far higher fatality rate than the flu by several orders of magnitude.
2. Everyone is at significant risk to die from this virus.
3. No one has any immunological protection, because this virus is completely new.
4. Asymptomatic people are major drivers of the spread.
5. Locking down—closing schools and businesses, confining people to their homes, stopping non-COVID medical care, and eliminating travel—will stop or eliminate the virus.
6. Masks will protect everyone and stop the spread.
7. The virus is known to be naturally occurring, and claiming it originated in a lab is a conspiracy theory.
8. Teachers are at especially high risk.
9. COVID vaccines stop the spread of the infection.
10. Immune protection only comes from a vaccine.
What if embedded in all of this is perhaps one more lie?
The greatest lie.
The one lie to rule them all.
This is the one that will come back to haunt us over and over if we do not call it out by name and lay plain its resounding lack of basis in fact.
It’s the lie they have been trying to sell for decades and failing (or at least having only moderate success and thus wreaking only moderate havoc).
It’s the one lie to rule them all. The one lie to rule us all. The truly big lie constituting a forest that has been lost for the trees and perversely therefore winds up being reinforced by the very debate about the little lies. And that lie is this:
Pandemics are dangerous to modern societies.
Because the fact is that they are not.
As was the case with the Spanish flu, perhaps the last truly high excess death global pandemic to bedevil humanity, much of the damage was done by horrible reactions. and the parallels may be more poignant than people realize.
One of the enduring causes of fear during the 1918 flu was the way that it seemed to be killing otherwise young and healthy people (especially soldiers) in a matter of days. They would be a bit, sick then suddenly die of massive organ failure and “wet hemorrhagic lungs.” The progression was incredibly fast, seemingly irreversible, and was stacking people who really ought to have been low risk in mortuaries like cordwood. This made risk, CFR, and IFR look horrifying and fear near universal.
If it could do this to a solider in his prime in a matter of days, every last one of us should be terrified.
But this is simply not a realistic outcome. In a modern society (even pre-antibiotics) it basically doesn’t happen. These are not the pre-sanitation/most people do not get enough calories days of the Black Death.
Diseases that kill at high percentages tend not to spread because killing the host is evolutionarily maladaptive. It’s like trying to conquer the world by burning down your own house and car. Even the really nasty historical killers like smallpox were only infecting ~400k people a year by the late 1800s and excursions above 1 death/year per 1,000 population during outbreaks were very rare not in spite of, but because the fatality rate was so high.
But respiratory diseases are different and tend to spread far more. Fatality rates are low. The claimed Spanish flu CFR was always suspicious in this regard. And there may be a reason:
There is actually quite a lot of convincing evidence that many of the “young, healthy deaths” in Spanish flu were iatrogenic. This is a word that’s going to come up a lot and a topic that’s going to be the big field of debate around covid going forward. It’s probably one of the most important scientific questions in the world right now. So let’s define it:
Loosely put, iatrogenic death is when the doctor kills you. And there is a long and unpleasant history on that one from Benjamin Rush bleeding George Washington to death to killing “witchy” cats to stop a plague carried by the fleas of the very rats they were eating to (and especially) new “wonder drugs” that are poorly understood but that rapidly go into widespread use.
And one of those drugs was aspirin.
Aspirin had just come into widespread availability in 1918 (and Bayer was rushing it to market for the pandemic). It was the new wowie-zowie drug and doctors (and especially militaries) all over the world fell in love with it. They prescribed it widely to those with Spanish flu. In doses ranging from 8 to 31 grams per day. Oopsie.
A typical aspirin today is 325mg and max dosing per day is ~4 grams.
A toxic dose is 200-300mg/kg of weight. That’s about 20g for a 180 pound person.
So 31g is “You’re going to die really, really fast and there is not a damn thing anyone can do to stop it once you take that dose.”
This is why incredible caution should be exercised around large departures from tested and true medical practice and new pharma modalities and products.
Stop me if any of this starts to sound familiar. (study HERE)
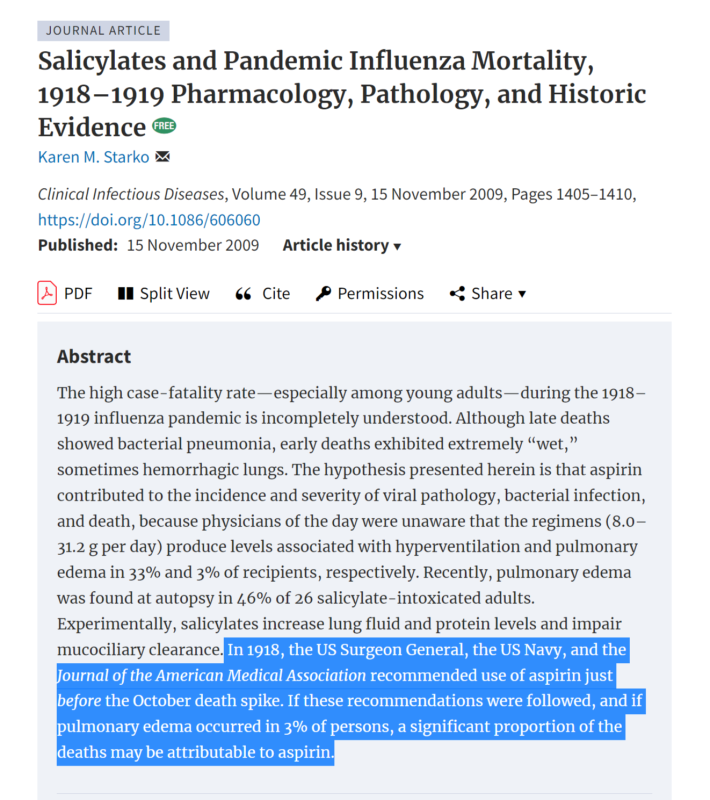
The unprecedented overall mortality and the mortality rate among young adults during the 1918–1919 influenza pandemic are incompletely understood. Deaths in the United States peaked with a sudden spike in October 1918. Later, Wade Hampton Frost [2] studied surveys of 8 US cities and found that, for every 1000 persons aged 25–29 years, ∼30% were infected with influenza virus, and 1% died of pneumonia or influenza. This 3% case-fatality rate has been called, “perhaps the most important unsolved mystery of the pandemic” [3, p 1022]
This case fatality rate has never looked even remotely plausible for flu. You simply do not get a respiratory disease like that in a modern (or possibly any) society, especially not in young, healthy people. It’s just not a thing.
But widespread poisoning by well-meaning medical professionals who have no idea how dangerous the products and procedures they are playing with is.
Official recommendations for aspirin were issued on 13 September 1918 by the US Surgeon General [64], who stated aspirin had been used in foreign countries “apparently with much success in the relief of symptoms” (p 13), on 26 September 1918 by the US Navy [29], and on 5 October 1918 by The Journal of the American Medical Association [31]. Recommendations often suggested dose regimens that predispose to toxicity as noted above. At the US Army camp with the highest mortality rate, doctors followed Osler’s treatment recommendations, which included aspirin [48], ordering 100,000 tablets [65]. Aspirin sales more than doubled between 1918 and 1920 [66].Again, anyone starting to pick up a bit of a rhyme in the history here?
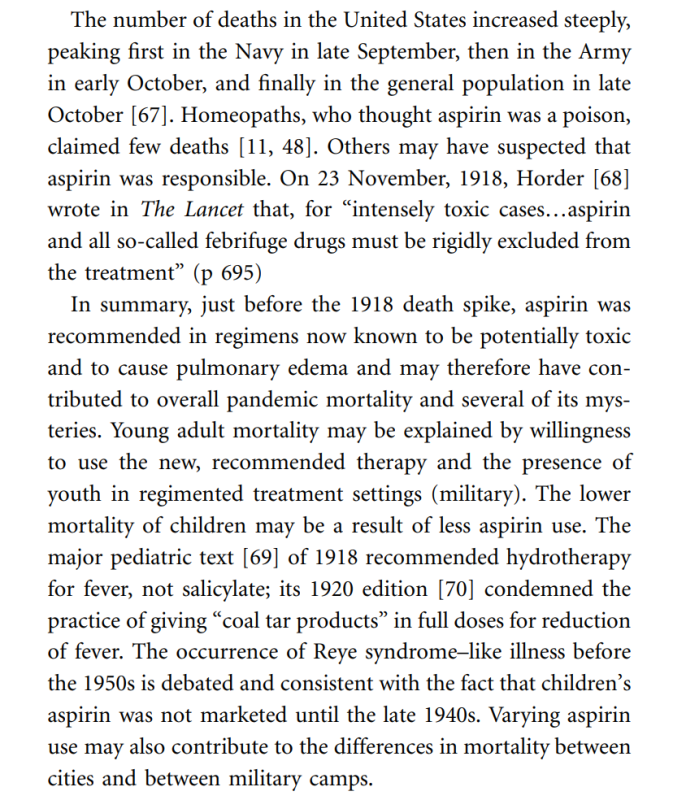
The similarities to recent events are more than a little striking. (Bold mine)
Autopsy reports by pathologists of the day describe extremely wet, sometimes hemorrhagic lungs in early deaths. On 23 September 1918 at Camp Devens in Massachusetts, 12,604 soldiers had influenza, and 727 had pneumonia; after examining the lungs of a dead soldier, Colonel Welch concluded, “This must be some new kind of infection or plague” [48, p 190]. What struck E. R. Le Count [49], consulting pathologist to the US Public Health Service, as most unusual was the amount of lung tissue actually “pneumonic” seemed “too little in many cases to explain death by pneumonia.” He saw a thin, watery, bloody liquid in the lung tissue, “like the lungs of the drowned,”
And as ever, bigger hammer theory tends to rise to the fore and the terrible tenet of “it’s not working so do it harder” comes into play.


love this
Very interesting blog post! It’s important to question the information and lies promoted by public health leaders, especially during pandemics. I was especially intrigued by the idea that pandemics are not actually dangerous to modern societies, and the comparison to the iatrogenic deaths during the Spanish flu. Do you think the current COVID-19 pandemic is also being affected by iatrogenic factors?
Nette
BestDogsStuff.com
LikeLike