1
2
3

4
5

6

7

8
9

10
11
12
13
14
15
16
Fish
The Best and Worst Fish to Eat: A Guide to Maximizing Benefits While Minimizing Toxins
Gross and Disgusting Air Travel
Shithole Cities
What the Hell Is Wrong With Charlotte? – I hate that city. I avoid it and drive around it every time I have to go near it.
Heatlth
Large Study Connects Sleep Apnea Risk with Declining Mental Health
Cars
Mapped: The Best-Selling Vehicle in Every U.S. State
UFC
UFC Fighter Throws Up After Getting Kicked In The Nuts At UFC 326
Masulinity
Men are back – we’ve figured otu that MeToo was mostly a lie as are trannies, and than Men are the better leaders. All women have is to try and tear down men instead of supportin gthem
Energy
$1.3 trillion savings: The impact of Trump dumping Obama’s ‘Endangerment Finding’ – ending another lie told by Obama screwing Americans
Obamacare
3 Reasons Why Obamacare Is So Hard To Fix – Premiums have more than doubled over 12 years. Some consumers have only a few plans to choose from. And flaws in the program’s design continue to waste taxpayer dollars.
The Retard Tampon Tim
It’s Official: Tim Walz’s 20-Week PAID Leave Program Now in Effect — Open to Illegals and Non-Citizens – While Trump was saving the country from drugs, Minnesota turns into a shithole
EU May Be the Next Retarded Economy
The EU imposes a €3 fee per package: more control, more revenue, and more bureaucracy at the consumer’s expense – next time they talk shit about the USA, remember this. They screw their own. They are going to break their own people.
Speaking of Retards
JUST IN: Kamala Harris Gets LIT UP on X After Blasting Trump’s Capture of Maduro – Imagine if she’d been president, she’d have no idea what to do, wouldn’t support the military, and the country would be even more rampant with drugs from Venezuela.
Cars
Red Bull unleashes final evolution of Adrian Newey-designed RB17
Uninformed Opinions That Don’t Count, Or Are From Retards
Growing Older And Smarter
Lifestyle Changes That Only Make Sense After 60 – well, I’ve done a lot of this
Walk Your Way to a Healthier Heart: How You Accumulate Steps Matters More Than the Total Step Count
Sports Betting And It’s Cost To The Game
Major sports leagues leaped into bed with gambling industry—now comes the cost…
Traitors
10 Times Democrats, Corporate Media Leaped to Defend Somalis Despite Massive Fraud Scandals – Hey, it’s their voter base and money laundromat.
Political Winners and Losers in 2025
8 political winners and losers of 2025 – finally a good year for the Country
Eating Out
Why restaurants and fast food suck
Fraud
Minnesota’s Somali Fraudsters Paid for Lamborghini, Rolls Royce Rentals, Luxury Resort in Kenya With Stolen Money – that’s our tax money, and there are real people who needed it to live. You effing icehole stole it with the help of the people who are running that place.
Artificial Intellingence
SURPISE! AI Emerges as the Biggest Driver of 2026 Inflation
The Gates of Vienna
40% of All Babies Born in Vienna Do Not Have an Austrian Passport – Doesn’t anyone remember stopping this once before?
Obamacare
Obamacare Was, Is and Will Always Be a Problem – just like the civil rights act of 1964, it was to swing votes to the left
Anne Frank’s Sister Dies at 96
Holocaust Survivor Eva Schloss, Stepsister of Anne Frank, Dies at 96
Cost of Somalian immigrants
Somali Immigrants Are Most Expensive On Earth… yes, but they are making the politicians rich
Election 2026
Both Parties Trying to Attract Young Male Voters in Midterms – because all the liberal white women are voting for socialism, and their own destruction. Someone has to save the country from them.
Flu
Cleveland Clinic Flu Shots Study Shows Vaccine INCREASED Risk of Getting the Flu – don’t ever get another vaccine until they stop lying about healthcare
What Men Do
Heroic Texas Father Rescues Kidnapped Daughter on Christmas Day by Tracking Her Phone – Suspect in Custody Without Bond – not that a liberal white woman would have had a child, but wouldn’t know how to save her. We need men. This guy is a hero
Wanker
King Charles Goes Full Woke: Parrots ‘Diversity Is Our Strength’ in Christmas Speech While UK Suffers from Migrant Mayhem – no wonder the UK has problems. Unity is our strength, not diversity. What a plonker. The UK needs William soon.
fafo
‘Blooper for the Books’ — Illegal Alien Arrested After Running Red Light, Crashing Into Federal Immigration Vehicle – time to move them all out
Ariticial Intelligence
How the AI Bubble Is Being Masked Within Big Tech – great if you are one of the magnificent 7, otherwise, not so great
Communism
The Con of Communism – We have to protect our country from liberal women voting in our country’s demise. Lenin would be right, convince the weak and he’ll take over in a generation.
Somalians
Minnesota Mayor Mike Murphy Says His City Can’t Even Make Their Own Water Because of Somali Fraud [VIDEO] – take them out of their shithole, move them to Minnesota and it becomes a shithole. Send them home
Real Estate
10 US Cities Where Home Values Are Up — And 10 Where They’re Down
Cars
EVs were a $30B loser for Ford… Thank you Joe Biden for showing us that this is not the way to go, plus people want a Hemi or something that loud and strong
We Lined up a 2006 Corvette Z06 Against America’s Wildest Tuners — Here’s Who Survived
This is the best they have?
Kamala Harris and Bernie Sanders Top Democratic Favorability Ratings; Gavin Newsom, Tim Walz Lagging – professional politicians and commies, not leaders
Survivor just took on a whole new meaning
Health
Unmasking the Great Ozempic Scam – the other side of the story.
Minnesota Fraud
Citizen Watchdog Went to 50 Somali ‘Daycares’ in Minnesota and Found Zero Kids There, Ever [VIDEO] Tampon Tim is a retard, Ilhan Omar is a thief, and the state has been taken for a ride
Formula One
Hamilton is Ferrari’s first new driver in 44 years to complete season without a podium | Formula 1 – When it’s time to retire. He was great when his car was a second a lap faster than everyone else,
Health
Microplastics: The Silent Brain Invader Fueling Neurodegenerative Diseases – how your brain is being destroyed, but some things you can do to prevent it.
The Bone Cost of Ozempic – you lose muscle and bone
1984
11 Signs That Our World Is Rapidly Becoming a Lot More Orwellian – UK, EU, France, India tracking everyone, digitital ID
Underground Cities
30 Hidden Underground Cities in America [VIDEO] – I guess they really were afraid of nukes, but sometimes it’s just to get to work.
Obamacare Fraud
Widespread Obamacare Fraud: Phony SSNs Had a 100% Success Rate for Getting Coverage, Investigation Finds – It wouldn’t happen if they didn’t plan it and let it happen. No wonder the average premium is skyrocketing. If you like your plan, you can keep your plan……right
Waiting for A $19,000 Shit, Crime.
Thief Swallows $19K Fabergé Egg: Police Wait Six Days for Suspect’s Expensive Bowel Movement
Cars
This Jaguar Build Crosses Lines We Didn’t Know Existed – Possibly the ugliest and worst car ever built. Get woke, definitely go broke and out of business if this is what they are trying to sell. Maybe a museum will get one to show what not to do.
Bad Food
‘I Wouldn’t [Feed] It to My Cat’: Vermont Woman Buys 4-Pack Of StarKist Solid White Albacore Tuna In Water. Then She Opens A Can – When anyone opens a can of tuna, it smells like a bait shop
2021 Afghanistan Pullout
Watchdog: U.S. Weapons Now Core of Taliban Military – One of the biggest military mistakes in history, brought to you by Joe Biden. Now, they are using them on us, FJB.
Taxpayer Money theft
“50 Percent of Supercars in Monaco All Had Ukrainian Plates” (Video) – In January 2022 news broke that Ukrainian officials blew millions of US taxpayer dollars in sports cars, mansions and luxury vacations.
There has never been an audit on the over $110 billion in US taxpayer dollars sent to Ukraine, one of the most corrupt nations on earth.
Climate Hoax
Most-Cited Climate Study Retracted – the hoax is starting to be over. Only those whose religion is climate change can ignore the facts now
Obamacare
Obamacareless: 90% of Fake Applications Approved, GAO Review of ACA Finds
How WWIII Will be fought
Experts Warn of Tool China Is Using To Play ‘Long Game’ in New Cold War – they don’t need nukes.
Cars
1970 Lamborghini Miura P400, 1 of 6 produced hitting the auction block
Toyota GR GT Revealed: Twin-Turbo V-8 Muscle Meets a Lightweight Aluminum Frame
1969 Ford Mustang Boss 429 Fastback – I will grab rubber in all 4 gears. A bad ass car
Artificial Intelligence
Nvidia CEO Stuns Rogan With Jaw-Dropping AI Prediction – The dark side of what AI can do
Health
Sugar Starts Corroding Your Teeth in Seconds but These Holistic Habits Can Mitigate the Damage – I didn’t know it was this bad, plus sugar in coffee is for pussies.
The Dangers of 5G: Health Risks, Privacy Threats and the Push for Resistance – maybe I’ll go back to a flip phone
5 Health and Insurance Moves Every Man Should Make This Year
creation
Anything but God?: Scientists “Seriously Asking” if Life on Earth Was “Seeded by Aliens” – Anything But God
Climate Hoax
Media doing ‘damage control’ as widely reported study on cost of climate change gets retracted – Now that the authors have retracted it, the flaws are being downplayed by the media – of course the media is lying, They rode that horse so long they actually believed it. Never trust them
“Instinctually Programmed To Lie”: CNN’s Jake Tapper Mislabels D.C. Pipe-Bomb Suspect As “White Man” – Stevie Wonder knew he was black. Jack Tapper is a liar. The press can’t help themselves from the narrative.
Terrorism
Afghan refugees killed 55 people, wounded 92 in U.S.: report – get them out of here
China
Alleged Chinese Spy Linda Sun Said Hochul was ‘Much More Obedient’ Than Cuomo – figures, Liberal White women
Pipe Bomber
FBI Pipe Bomber Breakthrough Exposes Biden Era Failures After Four Years – Biden Administration sat on it for 4 year
Education
Tiny Qatar Is Using a Trillion Dollars to Manipulate Education Across Western Society [VIDEO] – trying to tell us that Islam isn’t dangerous and other lies
1
2
3

4
5 – I’m laughing at the girls in NYC. They will pay for their act of treason.

6
7

8
8
9

10
11
12

13
15
16

17
18
19 – LIberals are 2 faced

Football
Here’s Why NFL Games Feel So Different Than in Years Past – They are boring. Bring back the gunslingers who could stay in the pocket and throw for 400 yards. Give me a young Dan Marino any day for excitement. I don’t think the running QB has helped anyone if you read the article.
Cars
2026 Dodge Charger Sixpack Sounds off but Drives Better Than You Think – Yes, but wouldn’t you rather have a Hellcat? The auction price ina couple of years will show that this isn’t the Charger you were looking for. Give me a Hemi any day.
Obamacare
Obamacare Is a Disaster, Just as Expected – prices up, service down, politicians get rich, insurance companies don’t care. Socialized medicine is never good, just ask Canada, UK or the EU. We were lied to the whole time, about everything. The stats are in the article.
The War on America
The Red-Green Alliance Is Still Powerful – still the most powerful military ever, but the war is from within, and unless Americans wake up, it will work. Stop the liberal White women and the socialists.
Mamdani, Debs, and the Rise of Democratic Socialism – for the record, the Nazi’s called themselves democratic socialists. Will someone learn history?
Cop30
COP30 to Clear-Cut30 to CRAP30! Week 1 Round-Up: UN urges delegates ‘not to flush toilet paper…in the toilets at the COP 30′ – Summit empowers China – Hamburgers sell out at UN! – Gore says Gates ‘Silly’ & fears Trump! How are we normal people supposed to believe these hypocrites? They aren’t even hiding the fact that this is about power and money.
CSM Upset That Trump Is Looking At The Climate Con While Xi Looks At Cash – Xi is exporting all the solar and wind crap he can, complete with spying technology. Like Al Gore, it’s about the money, not the climate.
Al Gore: Did Fear of Trump Force Bill Gates to Abandon Climate Activism? – No, the real question is who gives a shit what Al Gore thinks? No one has been a bigger liar about climate activism than this piss ant.
A terrible way to die
New Jersey: Pilot father is first documented death from meat allergy ‘caused by tick bite’
JFK – More of prick than we thought
JFK’s secret trailer park lover: The sex was so ‘wild’ that Kennedy let slip his marriage to Jackie was ‘ARRANGED’… now read the full story, revealed for first time in her bombshell unpublished memoir – He never loved anything but politics and snatch. Ruining others lives was just collateral damage.
SNAP
5,000 Dead People Getting SNAP; 500,000 Getting Benefits Twice: Rollins – drain the swamp and the fraud. Grifters need to go to work. Give to the needy, not the greedy.
Butt Hurt over shut down
“Incandescent Rage”: Far-Left Nonprofit Head Furious Over Democrats Caving To Trump And Ending Shutdown – well, we know who is behind the democrats and who is the half that hates America
F1
Ferrari leads F1 team valuations as billion dollar boom continues – $5.8 billion, more than most sports teams
Porsche
This Porsche 911 Targa Was Buried Under Pine Cones for 31 Years Until Now
Artificial Intelligence
AI Is the Inflection Point for Humanity
Marxism for losers
Blaming Boomers Is Generational Victimhood for Losers
Childish Humor While Being True
Today I Learned About The Last ‘Fart Lamp’ In London And You Should Too
Bastketball Records
The 9 Most Unbreakable College Basketball Records – Not any by the new 1 on 1 showboating types.
Problems with SNAP
Broken System: 500K People Get SNAP Benefits Twice, Plus 5K Dead People Are Still Getting SNAP [VIDEO] – fix this, get rid of the illegals and it will help the people needing help.
Artificial Intelligence
ChatGPT Is Full of Nonsense – of the engines I use, it’s easily the worst and most biased, but then it has a lot of Google in it so I’m not surprised.
Obamacare Built in Cost Increases
Sen. Fetterman On Affordable Care Act Subsidies: Dems ‘Designed Those Tax Credits to Expire’ – They knew they were screwing us from the start. Well Nancy Pelosi, you voted for it and we found out what was in it, screwing the American public
Liberal White Women
Gallup: Nearly 4 in 10 Young Women Want to Leave US – go then, you’ll be making both of our lives better. Gen Z guys are more conservative so they don’t want you either.
Arkancide
Clinton Body Count: Epstein Email to Disgraced Journalist Alleges Hillary Had Sexual Affair with ‘Suicided’ Vince Foster – so the evidence points at Hillary, but the real question is who would want to have sex with her?
Feminism ruining females
What Is Stealing Women’s Childbearing Years? – you go girl, have everything you want, until you realize life passed you by while you thought you were ruling the world
Pandora’s Box is open
Seattle’s New Socialist Mayor Goes Full Communist, Says She Won’t Allow Private Grocery Stores to Close – put a liberal white woman in charge and you are screwed.
Car Art
One-Off McLaren 750S Turns Las Vegas Into Automotive Art
Schadenfreude
Starbucks Workers Launch Strike on Chain’s Biggest Day of the Year – I have a Schadenboner. Maybe people that can’t afford it will stop buying that bat piss.
Food Scenes In Movies
Ranking The 16 Greatest Food Scenes In Movie History – I had food fight from Animal House as my number 1.
Nature
USA
America’s Real Enemy – and it will be hard to defeat
‘Oh, F*ck Off!’ Democrats Rage at ‘Pathetic’ Shutdown ‘Betrayal’ in Mass Backlash
“At What Point Does This Become Treason?”
Artificial Intelligence
How AI Is Supercharging Scientific Fraud
DOGE
DOGE: U.S. Government Agencies Terminate 67 Wasteful Contracts Worth $1.4 Billion
Communism
White House Declares ‘Anti-Communism Week’ Honoring 100 Million Lives Lost
Islam
‘I Beat Hitler’ – Survived Dauchau only to see the election in NYC
Cop30
UN’s Clear-Cut30: Morano on Real America’s Voice TV: ‘Brazil has clear-cut up to 8 miles of virgin tropical, Amazon rain forest at this summit…in order to bring in the private jets and the limousine’ – Hypocrisy, thy name is Climate change. Let’s not forget it started out as AGW. Antrhropogenic Global Warming. Humans didn’t do anything other than scam others for money. It was the same formula BLM used.
Government Shutdown
Speaker Johnson calls House back to end shutdown as Jeffries urges Democrats to oppose deal – because it cuts off the money laundering through the insurance companies back to the dems. They don’t care about insuring the people. It ends their control and push to socialized medicine.
Snow Skiing
Watch: The Greatest Ski Descent in History… Everest’s Stunning Hornbein Couloir… – There’s a dragon I don’t have to slay
Jobs
China’s DeepSeek Issues Rare Warning Of An Incoming AI-Fueled Jobpocalypse – it pays to be a carpenter or a plumber. office and administrative jobs are going to get the sword
Lying
Eric Swalwell Names Washington DC Home as ‘Principal Residence’ and Has No California Address – combine that with sleeping with Fang Fang, the Chinese spy and you have a real loser here.
Quantum Computing
Quantum Computers Model Complexity of Materials – It will challenge the limits of current computing and surpass it.
UK
‘A wicked wife’: The truth about Tudor England’s ‘most hated woman‘ – by the time I read it, I hated her also.
EV’s
Mercedes Slashes Prices by Up to $50,000 as EV Inventory Piles Up – Nobody wants them. Even Porsche is cutting back. The Ford F150 Lightning is dead also
Seal Team
SEAL Team 6 Operator Reveals High IQ Move To Kill Osama Bin Laden: WATCH – I never get tired of this story
Health
Study Finds That Common Dry Cleaning Chemical Tetrachloroethylene Linked to Severe and Potentially Fatal Liver Damage – all of those clean clothes killing people
China Spying
‘Wreak havoc’: U.S. nuclear bomber fleet shares fence with trailer park linked to Chinese intel-tied fraudster – No, they aren’t spying, they’re just running a trailer park
Islam Practices
Muslim Preacher Says Americans Are So Uncivilized and Backward That They Use Toilet Paper – back to 600 AD we go by starting in NYC and Minnesota. Stop it now so we don’t have to have a Gates of Vienna.
Obamacare
The Obamacare Secret at the Heart of the Shutdown: Insurers Made Billions at Taxpayer Expense – Lies, lies, lies from the start. It was always about the money and socialism, not healthcare.
Doctor Lays It Out So Clearly: Barry’s Affordable Care Act Was the Biggest Shakedown In US History…
Illegals
If You Move the Third World to the First World, Eventually We Become the Third World – Look at the UK, Rapes in Sweden, Germany Economy. Stop it at NYC now before it ruins the US.
Quantum Computing
Space: The Final Frontier – A financial opportunity for a technology searching for money.
Quantinuum Makes Another Milestone On Commercial Quantum Roadmap – Who has the advantage?
Media (and Lying, but then I repeat myself)
Trump may squeeze the boobs at the Beeb – Anti-Americanism at its’ best
Another How Woke and Feminism is ruining everything they touch.
Born Perfect: The Girlboss and the Death of Growth… – From ruining Star Wars to businesses. Why Luke Skywalker had to suffer to become a hero. Men had to learn to lead the hard way and this shows why the lessons have to be learned. You can’t just DEI your way to be a leader. 2 of my 3 worst managers were girls. They made life this difficult.
Double Standard for the Elite
“Clinton Corruption Files” – Bondi, Patel Give Congress New Evidence Detailing Clinton Foundation Corruption – They clearly not only broke the law, but mocked others. They’ll also get away with it. It’s like they have evidence on others that is blackmail.
Academia
The Dirty Secret Behind America’s “Best and Brightest”: The Foreign Cheating Scandal Academia Won’t Touch – Cheating in Ivy League schools, I’m shocked
Illegals
‘If you move the third world to the first world, eventually we become the third world’ – Look at Germany, Sweden and the UK.
Cars
One of 48 Original Ford GT40 Mk1 going to Auction at Mecum in Spring.

TV
Disney/ESPN Losing $30 Million/Week Amid YouTube TV Blackout, According To Industry Expert – And I’m missing Jeopardy and Football. At least I can see F1 on F1TV because the BBC coverage is on ESPN, and it sucks.
Sports
The 5 Times A College Basketball National Title Was Won On A Buzzer Beater Or Last-Second Shot
Life Outside Of Blue States
Workers Think Dems Are ‘Weak’ and ‘Woke’ – ignore flyover states at your own peril
The Media
“Terrible Thing For Democracy”: BBC Top Brass Out After Misleading Trump Documentary – Lying again? About Trump of all people? Why, I’m shocked

Climate Hoax Hurts Germans
Endgame For Germany’s Industrial Power Prices: Green Deal Failure Sparks Subsidy Spiral – just turn on the gas and coal. You blew up the nuke reactors, but save your economy, please.
Ivy League
Welcome to Harvard, Where Studying Is Now a Hate Crime – producing incompetence and automatons for years.
Islamic Immigration Invasion
1st Generation Lebanese-American Brigitte Gabriel Warns About Inbound Islamic Conquest in America [VIDEO] – They can outwait us as a strategy. They are trying to outbreed us and take over political positions like Mamadani instead of with swords. Then the swords will come out along with the burkas. It’s the strategy since 610 AD.
44% of First-Graders Do Not Have Sufficient Language Skills to Follow Lessons in Germany – instead of assimilating, they force their culture on the countries they invade by immigration
WWII Navy Veteran Sinks British Establishment – Veteran says WWII wasn’t worth it to have the life they live in the formerly Great Britain today. Mohammad is the most popular name now.
Germany Admits Trump Was Right on Borders After Taking in One Million Syrian Refugees
Obamacare
Sen. Mike Lee On Obamacare’s Effect on Health Insurance Costs: It ‘Makes Everyone Else Poor’ – Socialism by any other name is still socialism.
Here’s How Obamacare Really Works, and It’s Disgusting
Who’s in? Who’s out? The quantum industry chessboard just got reset as the government releases its list of which companies have ‘feasible’ approaches to the potentially world-changing tech.
Hollywood
Black hat worn by the Wicked Witch of the West in ‘The Wizard of Oz’ is going up for auction, Plus 2 different Ruby Slippers. Just a prop, but so was Darth Vader’s lightsaber, which brought in a ton of money
Civil War
What Do You Do When Your Neighbors Want You Dead? – As they said in Guardians of the Galaxy, kick names and take ass. I have one great neighbor and some wieners. I know I’m supposed to be nice, but there are a couple who’s asses I’d kick in an instant.
Investing
Forward Return And The Importance Of Math – maybe not a crash, but the market isn’t going to go up forever. Fundamentals mean everything.
Wine
Which Countries Drink The Most Wine? – It was who I expected.
Sex on a plane
Couple Have Sex Aboard Flight to Florida in Front of Mother and Children Won’t Be Charged With a Crime – she was giving him a hummer
Humor
Nature (can be brutal)
Video shows orcas hunting great white sharks and devouring their livers – And we thought the Great White was the Apex predator.
Healthcare
What to Know About Obamacare Rates for 2026 – Costs are going up for everyone, quality of service will go down for many. It was a lie from the beginning to move us to Socialized healthcare, a failure every time.
Rare Genetic Disorder Causes Portuguese Boy to Reek of Dead Fish Every Time He Eats Seafood – sounds like one of my ex girlfriends who became an ex very fast.
Police Save Child Held Hostage (warning: graphic video)
Florida Sheriffs Drop Knife-Wielding Assailant Holding Child Hostage With a Knife [VIDEO] – when good guys win and save the day.
College Education
More Americans Are Asking if College Is Really Worth It – indoctrination centers for socialism, maybe for very specialized degrees, but gender studies and the like are a waste if you want a job.
Media, or Lying, it’s the same
Whistleblower Reveals How World’s “Most Trusted” Broadcaster Doctored Trump Speech a Week Before the Election – Never trust the media, any of them. They rarely tell the truth and then only by accident.
Hollywood
Actress Jennifer Lawrence Admits Trump Derangement Is Pointless, and America Doesn’t Care What Hollywood Thinks – Wow, one of them actually sees the truth. No one cares what actors think. In fact, we wish they’d shut up about everything but acting.
NYC Election
Rabid Jew Hater, Linda Sarsour, Admits That Zohran Mamdani’s Rise Was Both Planned and Well-Funded – I can’t believe that NYC keeps finding a bigger loser than before to be mayor. If this guy gets in, the City that never sleeps will also be the city that never eats.
Technology
Google Caught Hiding Elon Musk’s Grokipedia, Promotes Leftist Wikipedia – Of course they did. Google censors everything not Google. They are the hemorrhoid on the asshole that is technology.
Senate
Report: Rep. Pelosi Will Not Seek Reelection – I guess insider trading paid off enough to retire. Who’s going to be the first to say the wicked witch is dead?
Quantum Computing
China’s First Atomic Quantum Computer “Hanyuan No. 1” Goes Commercial – Whichever country wins this race has a significant advantage, especially in AI
Jobs
IBM To Lay Off Thousands Before The End Of The Year – They always fuck over the employees right before the holidays
Obamacare
“Such a Scam!”: Watch Fed-up Woman Explain Realities of a Failed Obamacare – You’re just learning that now? It’s because you got freebies at first. Now, the truth comes out and people are pissed
Government Shutdown
Air Traffic Controllers Union Chief Blasts Schumer for Playing Politics With Nation’s Safety – Schumer owns this one
Snap
Black Men Say SNAP Benefits Are Hurting Americans [VIDEO] – Of course it is, and the Dems know it because they are behind it.
Great Britain
Britain In the Balance – Like a monstrous experiment in social engineering, the profoundly anti-patriotic immigration policy of New Labour has brought about demographic changes that, right from the outset, were intended to be irreversible.
Climate Scam
Bloomberg News: ‘After 10 Years and $10 Trillion, What Did the Paris Agreement Achieve?’ – ‘The answer is clear…it hasn’t succeeded’ but it is ‘building the momentum that the world needs’ – not a damn thing other than making the biggest loudmouths richer, at the cost to the taxpayers
Nude, Scorched ‘Mother Earth’ to Blast COP30 Over Meaty Menu – Brazilian actress ‘will lie naked to lay bare the hypocrisy of serving meat, dairy, & other planet-killing foods’ at UN climate summit – the only good thing to come out of COP30
Obamacare And Government Shutdown
Obamacare’s Chronic Conditions: Shutting Down Government and Propping Up Policy Failure
Health
‘Harvard Thinking’: Cancer is rising among younger people — why? – Gee, why isn’t anyone mentioning the Covid Jab?
27 Microbes Linked To Pancreatic Cancer, Major Study Finds
Men Far More Likely Than Women To Die By Suicide – Next time you want to talk about Male Toxicity or White Priviledge, there’s this. There’s your privilege.
New Mexico’s State Capital Santa Fe Turns off the Fluoride Tap – It’s poison, they should turn it off everywhere
College Admission Common Sense
Affirmative Action Ban Already Having Huge Impact at Top Colleges: Report – who would have guessed this would happen? At least we are back to meritocracy
FAFO
Mental Illness
Radical Left Lunatics – look at the list of violence
Education
How Gen Z’s Education Is Powering Mamdani’s Campaign
AIDEN BUZZETTI: Stop Blaming COVID-19 For Poor Student Math And Reading Scores – Blame the Rap culture and Parents not being there for their kids
Climate Scam
World Getting Fed Up With Europe’s Unsustainable Climate Sustainability Act – How much longer are they going to continue this hoax?
A Cautionary Solar Tale: Billions Wasted Thanks to a Rush to Market
Government Shutdown
Elon Tells Rogan the Real Reason Democrats are Prolonging the Government Shutdown…– buying votes now, are we?
Cybersecurity
Waking Up to Cybersecurity Chaos – one bad apple and the world is in chaos
DEI
University of Virginia Employees Admit DEI Programs Still Exist, Only Names Have Changed – They’re not going to give up the link to being communist, free money and the minority vote that easy.
Victimhood
Michelle Obama Says America Did Not Show Her Family ‘Grace’ Because They Were Black (VIDEO) – What a crock of shit. She drank (a lot of) top shelf liquor, soaked the taxpayers for mega-millions for vacations, got on the cover of magazines for no reason other than being black. It sure wasn’t because she deserved it or looked good. The press protected and promoted her and now she has 3 mansions so that she doesn’t have to live with Barry. What an entitled person. Give us all a break.
Economy
America’s Power Bill Crisis Rages In Democrat-Run States – cut their taxes and watch the bills come down and people spend more.
Sports
Ranking the 10 Greatest High School Football Teams of All Time – Anytime you do these rankings, you piss someone else off. Everyone has their own opinion.
When they were trying to pass the Affordable Care Act, Obamacare, Bill Clinton talked to the Democrats. He told them you may not like it, but it’s the chance to get our foot in the door that will never be closed (my version of his words, but accurate as to his intent). In other words, we’ll work on it later to achieve what we really want, regardless of the initial outcome, just pass the damn thing.
Read this and judge for yourself if the promises came true and did Obama lie to the American public to sell it. Let’s not forget, if you like your plan, you can keep your plan. If you like your doctor, you can keep your doctor.
In July 2012, when campaigning for reelection, Obama repeated his assertion that—once implemented—the Affordable Care Act would reduce prices.
Running for his first term in 2008, then-Sen. Obama said he would sign a health care bill in his first term as president “that will cover every American and cut the cost of a typical family’s premium by up to $2,500 a year.”
In 2012, he spoke similarly about the law that had passed—with no Republican votes in Congress—but had not yet gone into effect.
“You should know that once we have fully implemented, you’re going to be able to buy insurance through a pool so that you can get the same good rates as a group that if you’re an employee at a big company you can get right now, which means your premiums will go down,” Obama said, when speaking in Cincinnati campaigning for a second term.
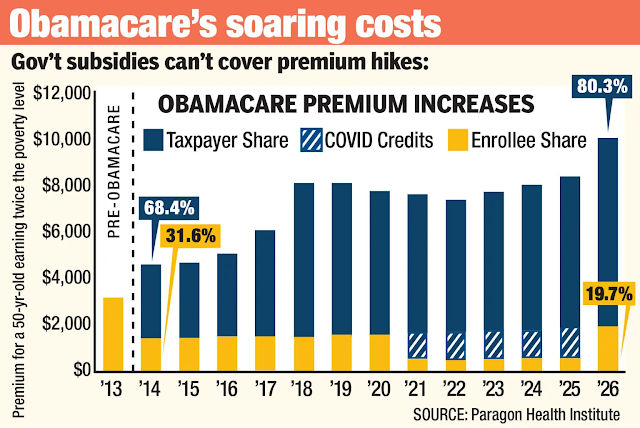
In 2013, when implementation of the Affordable Care Act began, the average premium paid by consumers in the individual market was $244 per month. By 2022, that cost had soared to $568 per month, an increase of 133%, noted a Heritage Foundation report from August 2024, “Key Health Care Trends: Nationally and in Each of the States.”
“The average deductibles for bronze-level plans sold on the exchanges increased by 40 percent between 2014 and 2024,” the Heritage report explains. “For self-only coverage, the average deductible was $5,094 in 2014, but is $7,144 in 2024, while the average deductible for family coverage has increased from $10,278 in 2014 to $14,310 in 2024.”
In recent years, 15 states have obtained federal waivers from some Obamacare provisions, which enabled insurers in the waivered states to reduce premiums.
The per-capita average monthly cost of individual market coverage had more than doubled in 40 states. In Missouri, costs had risen by 213%; in Alabama, by 309%; and in West Virginia, up 323%, according to the August 2024 Heritage Foundation report.
Obama asserted in October 2013 that the Affordable Care Act would create a more competitive insurance marketplace.
“What we’ve done is essentially create a competition where there wasn’t competition before,” Obama said. “We created these big group plans, and now insurers are really interested in getting your business. And so, insurers have created new health care plans with more choices to be made available through these marketplaces.”
But two-thirds of states, or 34 states, and the District of Columbia, had fewer insurers offering exchange coverage in 2024 than a decade earlier, before the Affordable Care Act was implemented.
On the slight upside, eight states had more insurers offering plans on the Healthcare.gov exchanges in 2024 than they had before the Obamacare law was passed, while eight others have the same number.
For 2026, some 183 qualified health plans are available on the Obamacare exchanges, the Centers for Medicare and Medicaid Services announced Wednesday. Of the 30 states using HealthCare.gov, 19 have more plans than the previous year, according to CMS.
That’s still substantially less than before Obamacare was implemented. In 2013, almost 400 insurers were offering coverage in individual markets at the state level before the ACA was implemented. Eight states had only one insurer providing insurance.
In 2026, 95% of enrollees will have access to three or more qualified health plan issuers. That’s down marginally from 96% in 2025, but an improvement from 68% in 2020, according to CMS. Fewer than 1% of 2026 enrollees have only one available issuer on the exchanges.
“Any potential benefits of competition were offset, or more than offset, by a subsidy design that really insulates enrollees from a lot of the cost, because the subsidies go up as premiums go up. That’s part of why you have seen the increase,” Ed Haislmaier, a senior research fellow with the DeVos Center for Human Flourishing at The Heritage Foundation, told The Daily Signal.
Obama said in September 2009, “I will not sign a plan that adds one dime to our deficits, either now or in the future.”
The initial score by the Congressional Budget Office in 2010 estimated the legislation would reduce the federal deficit. However, the cost of Medicaid expansion was higher than projected, as was the cost of subsidies, which was exacerbated by the COVID-19 pandemic.
The expansion of the COVID-19 era subsidies were passed as part of the 2021 American Rescue Plan Act and extended as part of the 2022 Inflation Reduction Act. The COVID-19 emergency formally ended 2-1/2 years ago.
The CBO found in 2024 that extending the COVID-era subsidies permanently would result in a $380 billion cost increase to taxpayers over the next 10 years.It would also likely mean 6.9 million individuals would be added to the Obamacare exchanges—receiving an average subsidy of $5,370 each. But of that 6.9 million, at least 3.5 million would be shifting from existing insurance plans such as employer plans, according CBO.
Before the COVID-19 subsidies, Obamacare enrollment was stable. In 2019, 13.7 million individuals drew a subsidy. By just the first quarter of 2025, that reached 26.7 million—nearly double.
“Obamacare is not affordable, and has narrowed network plans to exclude certain doctors and hospitals,” Brian Blase, president of Paragon Health Institute, a health care think tank, told The Daily Signal. “The only people purchasing are for the most part getting giant subsidies. It’s good for the health insurance companies. There used to be a guaranteed customer base with the individual mandate, which was eliminated. But it’s still a heavily regulated market, which decreases competition, and they receive massive subsidies.”
“The insurance reforms rest on everybody having access to coverage, and you also don’t do anything about the fact that taxpayers currently end up subsidizing the uninsured when they’re forced to go to the emergency room for care, to the tune of about a thousand bucks per family,” Obama said in March 2010. “You can’t get those savings if those people are still going to the emergency room.”
Almost 20 million newly eligible able-bodied adults enrolled in Medicaid from 2013 to 2023. That’s compared with Medicaid enrollment for children that increased by just 2.5 million, and for the elderly that increased by 1.2 million over the same 10-year span. The number of disabled enrollees over that period declined by 400,000, the Heritage Foundation report from August 2024 says.
Emergency room visits from the new Medicaid enrollees have increased, the Paragon Health Institute noted in a report last October.
“As a result of expansion, existing Medicaid enrollees have had more challenges obtaining doctor appointments,” the Paragon report says. “According to a 2019 meta-analysis, prior to expansion, Medicaid enrollees were half as likely as those with private insurance to get appointments, while they were only one-third as likely after expansion—a decline by one-third.”
From 2013 to 2023, Medicaid enrollment, as well as enrollment in the Children’s Health Insurance Program, soared overall from 61.1 million to 85.4 million.
Medicaid enrollment more than doubled over those 10 years in Alaska, Virginia, Oregon, and Nevada.
Deep State
Covering Up the Biggest Political Scandal in U.S. History
Healthcare
You Can Draw a Direct Line From the Failures of Obamacare to Today’s Schumer Shutdown
The Nobel Prize in medicine goes to 3 scientists for work on the human immune system – Don’t get a Covid jab
Liberal Men, Or Pussies…Same Thing
Liberal “Husband” Who Took Wife’s Last Name in Viral Video Is Actually, Well, You Know
The FDA Is Now Reporting That Some Imported Spices May Be Radioactive, Just Like the Shrimp
Legal
Energy
Education
Harvard Faculty: School Is Losing Its Competitive Focus – It lost it a long time ago
Another black lady college president exposed as massive plagiarist… BWBB
Sports
NFL roundup: Broncos knock Eagles from unbeatens with furious comeback – The 72 Dolphins are still the only undefeated team, again.
Health
HHS Resurfaces Old Tylenol Post Warning Pregnant Women NOT to Use Their Product
“Ivy League” Doesn’t Mean Excellent Medical Schools, According to New Index
Obama Defends Tylenol, Gets Wrecked in Replies – Even Tylenol recommends not taking it when pregnant, Obama is a hack
India, China, Europe, & The US Are On Very Different Population Paths
US
Spending run amok: Obamacare poisoning federal budget negotiations as shutdown looms
Q2 GDP Revised Sharply Higher To 3.8%, Best Quarter In Two Years
Three Muslims Arrested for Shooting Houston Youth Baseball Coach During Pregame Prayer With Children
Leaked Delta Force Hostage Rescue Video Goes Viral, Will Terrify Bad Guys
Sisters Who Trashed Charlie Kirk Memorial Now Whining They’re Jobless as They Beg for Cash Online – Karma is a bitch
Hegseth Eliminates One of the Root Causes of “Woke” in the Armed Forces
Tony Hawk’s Skateboard During His Most Iconic Run Sells At Auction For Double Presale Estimate
CarMax Shares Crash Most Since Dot-Com Bust
Space
European engineers develop a tumbling rover design moved by the Martian wind
Asia
Tokyo takes the top spot in ‘world’s coolest’ neighborhood rankings…
Europe
Europe’s Top Causes Of Death, Ranked; Cancer Is #2
World
Which Cities Have The Most Expensive Rent In The World?
A couple from the UK has signed up to die together in the Sarco “suicide pod” in Switzerland, and their deaths will allegedly be filmed.
Peter Scott (86) and Christine Scott (80) contacted the assisted suicide group “The Last Resort” last year regarding the Sarco machine because they wanted to commit suicide together after Christine received a diagnosis of vascular dementia — dementia caused by reduced blood flow to the brain.
But it wasn’t the diagnosis that worried them; what they fear is that neither of them will receive prompt treatment for their health conditions through the National Health Service (NHS).
“The chances of getting prompt NHS treatment for the ailments of old age seem pretty remote, so you end up trapped by infirmity and pain,” said Peter.
He told News.com.au, “We have had long, happy, healthy, fulfilled lives but here we are old and it does not do nice things to you. The idea of watching the slow degradation of Chris’s mental abilities in parallel to my physical decline is horrific to me.”
Rather than live out their lives, the couple will enter the Sarco pod — a device that, at the push of a button, will release nitrogen into the air, reducing the oxygen. They will die from hypoxia. According to Inspire, their deaths will be “filmed and provided to a coroner as evidence, setting a historic precedent in the field of assisted dying.”
All the reason you want right there on why state run (or socialist) healthcare is not our friend and is a recipe for death, if by incompetence as much as intention
“Trust me, I’m a doctor” is a humorous expression that suggests one’s opinion should be accepted without question, regardless of whether the person offering the opinion has actual medical expertise or experience.
The assumption is that physicians are knowledgeable, competent, and trustworthy. At one time, few would have questioned that assumption.

Image via Grok
In 2013, Rasmussen Reports surveyed American adults and discovered that a significant majority, specifically 81%, trusted their doctor.
Four years later in 2017, that number was even higher, with 93% of patients trusting their regular doctor.
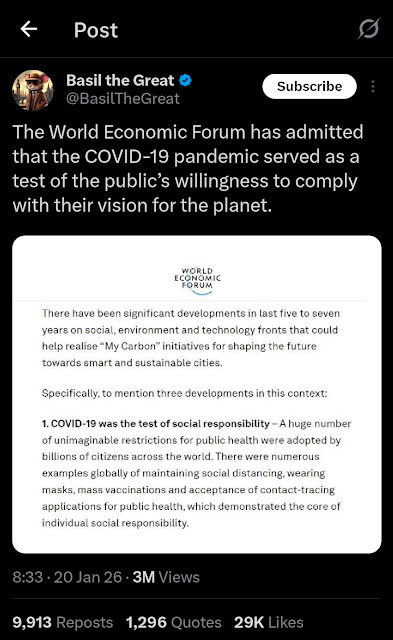
A funny thing happened in late 2019 and early 2020. In late 2019, almost no one had ever heard of COVID, coronavirus, or Wuhan.
The World Military Games were held, of all places, in Wuhan, China, in October 2019. A Department of Defense report from 2022 suggested that seven military members might have become infected with COVID-19.
We are only hearing about this now, two and a half years later. Apparently, this report was concealed among the Epstein files or Hunter Biden’s and Anthony Weiner’s laptops. However, the Biden administration covered up this report, just as they obscured their boss’s mental state and cognitive decline for four years.
Lies and coverups are a great way to destroy trust.
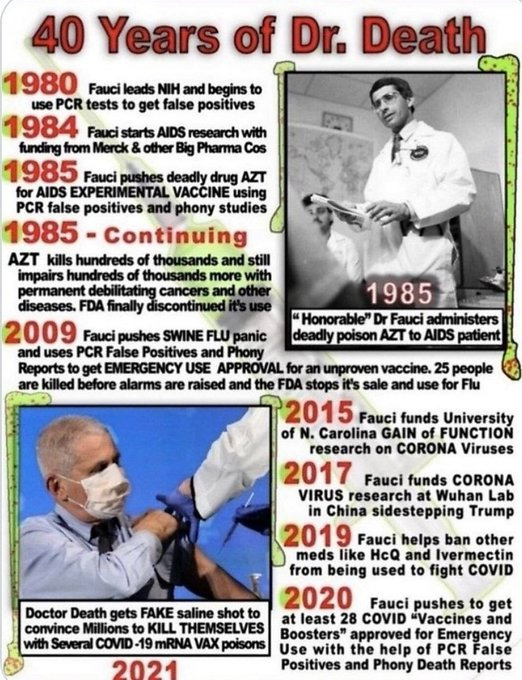
Dr. Anthony Fauci and his cabal lied to the public about the origins of COVID with their nonsensical “proximal origin” theory.
Why? To discredit President Donald Trump, who blamed China, and to conceal their illegal gain-of-function research.
Additionally, it may have been to maintain and protect money flow from China to the pharma-industrial complex.
This is one reason why trust in doctors and the medical profession has declined sharply over the past five years. You don’t have to take my word for it; I live and work in this new world of dwindling trust and observe it all around me.
The Journal of the American Medical Association conducted a survey of nearly half a million American adults across all 50 states and found, “The COVID-19 pandemic has been associated with a continuing decrease in trust in physicians and hospitals, which may necessitate strategies to rebuild that trust to achieve public health priorities.”
The Wall Street Journal, taking a break from criticizing President Trump over immigration and tariffs, noticed the declining trust in doctors. This past February, they published an article questioning, “Why we don’t trust doctors like we used to.”
They referenced a Gallup survey that stated, “Americans’ ratings of US professions stay historically low.”
In other words, it’s not only doctors who are held in low esteem but much of the administrative class as well.
Interestingly, another group of healthcare professionals topped the list, “Three in four Americans consider nurses highly honest and ethical, making them the most trusted of 23 professions rated in Gallup’s annual measurement.” Those surveyed must have missed the incessant TikTok videos of nurses dancing in ICUs during COVID.
And to no surprise for anyone engaged in politics and the news, “The least trusted professions, with more than half of U.S. adults saying their ethics are low or very low, are lobbyists, members of Congress and TV reporters.”
But it’s doctors falling most rapidly from grace, “About 53% of those polled in 2024 gave a high or very high rating to medical doctors, down from 67% in 2021. It’s the biggest drop among 23 professions ranked by Gallup in that period.”
There are many reasons. The WSJ offered a partial explanation:
People are increasingly wary of a healthcare system that is supposed to make them feel better but instead leaves them stressed and frustrated. And while much ire is directed at insurance and pharmaceutical companies, doctors are the front face of the system and are losing the public’s confidence, as well.
However, they overlooked the elephant that entered the room in late 2019, an elephant named COVID.
Consider the business and school lockdowns that closed churches while allowing strip clubs and liquor stores to remain open. It was illegal to surf alone in the Pacific Ocean, yet thousands marching together on city streets in the name of BLM or Antifa were considered perfectly safe and healthy.
Masks were deemed ineffective at protecting against tiny viruses until they were mandated as effective and lifesaving. As Dr. Anthony Fauci acknowledged, social distancing was arbitrary; “It sort of just appeared.” How’s that for science? As Gomer Pyle would say, “Shazam, shazam!”
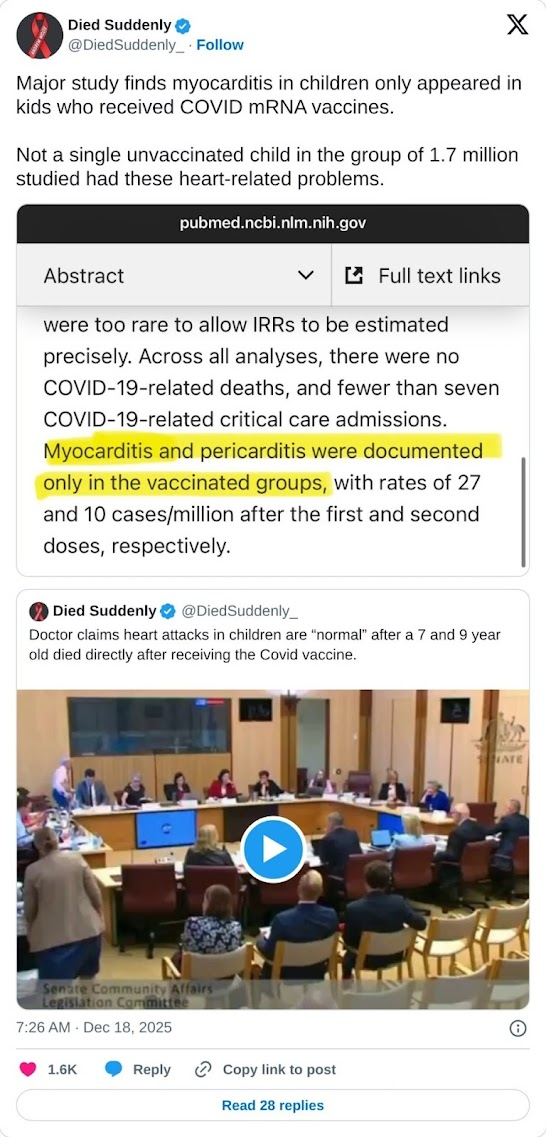
The vaccines proved to be neither safe nor effective. Otherwise, we wouldn’t be hearing about sudden deaths, blood clots, or myocarditis. Additionally, those vaccinated and boosted would not continue to contract COVID. Or as a Cleveland Clinic study found, the chance of getting COVID increased with an increasing number of vaccine doses and boosters.
Children lost years of education and social interaction to avoid catching a viral illness that posed virtually no risk of death to children. Jobs, businesses, and livelihoods were devastated due to political motivations rather than medical science. What impact does this have on trust in the medical system?
The U.S. healthcare system is failing Americans. The Commonwealth Fund reports, “The US spends the most on healthcare but has the worst health outcomes among high-income countries.” In most businesses, this would signal a death knell.
Then, there is the dysfunctional medical payment system, a combination of government and corporate control, which separates patients as consumers from physicians and hospitals as providers.
The Medicare fee schedule, which serves as the basis for all third-party insurance payments, will reduce reimbursement by 3% in 2025. This marks the fifth consecutive year of payment reductions, even as the cost of providing care continues to rise.
Physicians are compelled to see more patients throughout their workday, which results in spending less time with each individual and longer waits for appointments or to see the doctor during a brief office visit.
Patients are understandably frustrated and now see a doctor’s visit similar to a DMV trip.
The loss of trust extends beyond doctors; it includes the entire healthcare system, encompassing government-run health agencies and insurance companies.
The public has been overwhelmed by a continuous influx of misinformation, especially concerning the COVID pandemic, and has encountered censorship for asking questions or expressing complaints. Americans have been made to believe that our healthcare system is the best.
Although the system may benefit certain patients in particular situations, we fail spectacularly on a population level. Practicing medicine is no longer a calling or profession; instead, it has become a people-facing service trade influenced by price controls and an increasing number of rules and regulations.
Any private sector business operating in such a manner would quickly go out of business.
Trust lost is difficult to regain. Through transparency and disclosure, Robert F. Kennedy, Jr. may step in the right direction.
However, the basic structure of the healthcare delivery system is deeply flawed, and elected officials have no interest in undertaking the major reforms necessary to right the ship.
Healthcare spending in the U.S. exceeds $5 trillion, accounting for 18% of GDP, and continues to grow each year. Meanwhile, life expectancy in the U.S. is declining, and chronic diseases are on the rise.
Physicians who observe and voice any concerns may face censorship or threats to their medical licenses or employment. I experienced such backlash from the medical-industrial complex during the pandemic.
Clearly, what we are doing is not working, yet we are following the definition of insanity — doing the same thing repeatedly and expecting a different result.
It’s no surprise that fewer Americans trust the healthcare system. The phrase “Trust me, I’m a doctor” is fading into obscurity like another ridiculous saying from the past: “More doctors smoke Camels than any other cigarette.”
We must be able to trust our doctors with our lives and well-being. Can we still do that?
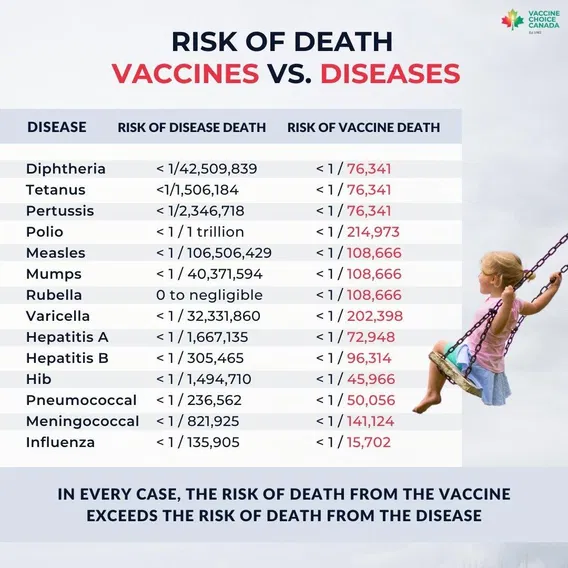
Two decades ago, CBS aired a bombshell report on the flu shot, revealing a truth that health officials didn’t want to admit. Despite flu shot uptake among seniors skyrocketing from 15% to 65%, flu deaths continued to climb. It doesn’t fucking work and the whole thing is a farce.

NIH scientists were devastated. They expected the data to confirm the vaccine’s effectiveness. But instead, their own research shattered that assumption. So they assumed other factors must be “masking the true benefits of the shots.”

Image Credit: Shutterstock / Mr. Nikon
However, as
Sharyl Attkisson reported at the time, “No matter how they crunched the numbers, they got the same disappointing result. Flu shots have not reduced deaths among the elderly.”
Atkisson, the reporter in the above clip, later left mainstream news to become an independent journalist focused on exposing Big Pharma, government corruption, and mainstream media lies.
Going back to the story, the scientists looked at the flu shot data of other countries in hopes of finding more optimistic data. But what they found instead was “the same poor results in Australia, France, Canada, and the UK.”
There are 8 in this article, but there are many more out there. Ivermectin and Hydroxychloroquine stopped Covid-19. We had Viet Nam won at the Tet Offensive except Walter Cronkite lied. Men can’t become women either. The Covid vaccine was safe and effective and preventing transmission or getting Covid-19. Obamacare, say no more there. I did not have sexual relations with that woman. One of the biggest is in the title, the mainstream media lies, all the time.
Here goes:
The mainstream media is in the habit of labeling something a “conspiracy theory” whenever they are attempting to discredit a particular point of view. Of course, such “conspiracy theories” have been proven to actually be true time after time. Meanwhile, the mainstream media has been caught in lie after lie in recent years. As a result, trust in the media is the lowest that it has ever been in the entire history of our country. At this point, most people realize that our largest media outlets are going to push the agenda of the globalists that own them, and they are going to be extremely hesitant to expose the big pharmaceutical companies and other giant corporations that spend billions of dollars to advertise on their networks.
The good news is that we have entered a period of time when the truth is coming out about so many things. The American people are now demanding transparency and accountability from major institutions throughout our society, and that is a wonderful thing. It is especially gratifying to see the mainstream media publicly admit mistakes that they have made. The following are 8 “conspiracy theories” that the mainstream media has been forced to admit are actually true…
For years, we were told that the lab leak theory was just “disinformation”. Of course now it has come out that certain individuals in very prominent positions waged a relentless campaign to discredit it. They were desperate to keep a lid on what really happened, but now the truth has come out. In fact, at this point even the CIA is publicly admitting that it is more likely than not that the lab leak theory is accurate…
The CIA has shifted its stance about the origin of the virus that causes Covid-19, NBC News reported on Saturday. The intelligence agency now believes that the coronavirus escaped from a Chinese lab, a shift from its previous stance, in which it did not take a position.
“CIA assesses with low confidence that a research-related origin of the COVID-19 pandemic is more likely than a natural origin based on the available body of reporting,” a CIA spokesperson said in a statement to NBC News.
For decades, anyone that went on the air and talked about MKUltra was considered to be a nut.
But now hundreds of government documents prove that this CIA mind control program really did exist…
Newly compiled records are spilling the beans on one of the CIA’s most notorious and shadowy programs: MKUltra, a wild attempt to develop mind control techniques through drugs, hypnosis, and psychological manipulation.
The collection was published by the Digital National Security Archive of The George Washington University in December 2024, detailing more than 1,200 documents on the CIA’s foray into behavioral and mind control experiments from 1953 until the 1970s.
Much of the information comes from records gathered by John Marks, a former State Department official who initiated the first Freedom of Information Act requests on the topic and authored the 1979 book The Search for the Manchurian Candidate.
We are actually very fortunate that these documents still exist, because in 1973 the director of the CIA specifically ordered that all records related to MKUltra must be destroyed…
In 1973, the director of the CIA, Richard Helms, ordered that all documents related to MKUltra be destroyed. However, a cache documents was discovered following a freedom of information request in 1977, which led to Senate hearings. MKUltra was declassified in 2001.
For ages, authorities insisted that putting fluoride in our drinking water was good for us. But now a federal judge has ruled that there is evidence that fluoride in the water could harm the intellectual development of our children. The following comes from CNN…
A federal judge has ordered the US Environmental Protection Agency to further regulate fluoride in drinking water because high levels could pose a risk to the intellectual development of children.
US District Judge Edward Chen cautioned that it’s not certain that the amount of fluoride typically added to water is causing lower IQ in kids, but he concluded that mounting research points to an unreasonable risk that it could be. He ordered the EPA to take steps to lower that risk, but didn’t say what those measures should be.
Over the past several years, the mainstream media has actually begun reporting on all of the nasty things that are showing up in the water that is coming out of our taps.
In fact, a study that was conducted in 2019 actually found 22 separate carcinogens in our drinking water…
For a lot of years, many of us in the alternative media have been talking about the “dumbing down” of America, but the mainstream media has continued to defend our system of education.
Unfortunately, it has become exceedingly clear that our kids are not alright. The following comes from the Wall Street Journal…
The reading skills of American students are deteriorating further, according to new national test scores that show no improvement in a yearslong slide.
The 67% of eighth-graders who scored at a basic or better reading level in 2024 was the lowest share since testing began in 1992, results from a closely watched federal exam show. Only 60% of fourth-graders hit that benchmark, nearing record lows.
The declines started before the pandemic, continued during it, and have persisted since.
For decades, alternative health practitioners and “conspiracy theorists” have been asserting that negative reactions to prescription drugs are one of the leading causes of death in the United States. Thankfully, the mainstream media has been forced to admit this as well. The following comes from a Vanity Fair article entitled “Deadly Medicine“…
Prescription drugs kill some 200,000 Americans every year. Will that number go up, now that most clinical trials are conducted overseas—on sick Russians, homeless Poles, and slum-dwelling Chinese—in places where regulation is virtually nonexistent, the F.D.A. doesn’t reach, and “mistakes” can end up in pauper’s graves?
Many of us have been warning about aspartame for ages, but the mainstream media just kept defending it. Well, after reviewing the evidence the International Agency for Research on Cancer was forced to classify aspartame as “possibly carcinogenic to humans”…
Assessments of the health impacts of the non-sugar sweetener aspartame are released today by the International Agency for Research on Cancer (IARC) and the World Health Organization (WHO) and the Food and Agriculture Organization (FAO) Joint Expert Committee on Food Additives (JECFA). Citing “limited evidence” for carcinogenicity in humans, IARC classified aspartame as possibly carcinogenic to humans (IARC Group 2B) and JECFA reaffirmed the acceptable daily intake of 40 mg/kg body weight.
Did you know that hundreds of Nazi scientists were smuggled out of Germany and brought to the United States in the aftermath of World War II?
And did you know that many of those scientists were used “to help develop America’s arsenal of rockets and other biological and chemical weapons”?…
As World War II was entering its final stages, American and British organizations teamed up to scour occupied Germany for as much military, scientific and technological development research as they could uncover.
Trailing behind Allied combat troops, groups such as the Combined Intelligence Objectives Subcommittee (CIOS) began confiscating war-related documents and materials and interrogating scientists as German research facilities were seized by Allied forces. One enlightening discovery—recovered from a toilet at Bonn University—was the Osenberg List: a catalogue of scientists and engineers that had been put to work for the Third Reich.
In a covert affair originally dubbed Operation Overcast but later renamed Operation Paperclip, roughly 1,600 of these German scientists (along with their families) were brought to the United States to work on America’s behalf during the Cold War. The program was run by the newly-formed Joint Intelligence Objectives Agency (JIOA), whose goal was to harness German intellectual resources to help develop America’s arsenal of rockets and other biological and chemical weapons, and to ensure such coveted information did not fall into the hands of the Soviet Union.
I could list many other examples, but I think that you probably get my point by now.
Just because something is labeled a “conspiracy theory” does not mean that you can automatically dismiss it.
In fact, many of those that love to accuse others of spreading “disinformation” are some of the biggest liars of all.
In this day and age, it is so important to think for yourself and it is so important to know why you believe what you believe.
Let me give you a piece of advice that really helped me.
Question everything.
Hold on to what is true, and discard what is false.
We live at a time when deception is running rampant, and it is getting worse with each passing day.
If you like your doctor, you can keep your doctor. If you like your plan, you can keep your plan.
He looked right at us knowing he was lying and lied to the entire country.
To begin with, it’s a Marxist idea and very few ideologies in history have killed more people than Marxism.
Specifically, this is what is happening.
I’m old enough to remember when health insurance was affordable. It wasn’t all that long ago; it was before Obamacare passed. Despite being officially called the Affordable Care Act, nothing about it has made health insurance more affordable. The question is, for the higher premiums and larger deductibles we have, are we even getting better coverage? The answer, which shouldn’t shock you, is a big fat “no.”
That’s right, despite paying more, you are also getting less. Health insurance denials and delays have hit record highs, and while many point the finger at insurance companies, accusing them of prioritizing profits over care, they’re not to blame. As Betsy McCaughey points out, the real culprits are the politicians who sold us Obamacare on a pile of lies.
“In 2013, before Affordable Care Act regulations kicked in, insurers denied roughly 1.5% of claims, according to the American Medical Association,” McCaughey points out. “But under ACA rules, denials increased tenfold. Now nearly 15% of claims are denied,” and some insurers are denying a third or more of claims.
Doctors and patients aren’t just battling denials — they’re also tangled in a bureaucratic nightmare of preauthorizations. As McCaughey notes, these delays force doctors to get insurer approval before providing care. And here’s the kicker: the person giving the green light is often unqualified to make those decisions. The AMA warns that an OB-GYN might be the one overriding your neurosurgeon’s recommended treatment.
And the consequences can be deadly.
McCaughey cites the example of a doctor who had a patient with metastatic breast cancer who needed a specific drug combination. But thanks to prior authorization delays, she had to settle for standard chemotherapy, which failed, and the patient died.
Obamacare is killing people.
It’s not just anecdotes. A House Committee on Energy and Commerce investigation found that Cigna overturned 80% of its Medicare Advantage preapproval denials upon appeal, proving that legitimate care is being withheld. And, as McCaughey reports, Cigna’s algorithm, PxDx, denies authorizations in bulk without considering individual cases.
If you like your doctor, you can keep your doctor. If you like your plan, you can keep your plan. That and everything else that came out of his mouth was an effing lie.
The shooting of United Healthcare’s CEO, Bryan Thompson, has engrossed the public. The shooting itself was a well-planned and audacious act. But when police apprehended the handsome, Ivy League-educated killer, many were disappointed. They were rooting for him to escape.
The killing has proven more popular than I would have expected. Moreover, this popularity is not confined to the left wing. People across the spectrum have shared their frustrations with the healthcare system and found themselves sympathetic to the killer.
An All-American Murderer
When Luigi Mangione’s background and manifesto were revealed, he appeared to have a good life and a promising future. His social media suggested an intelligent freethinker, whose views and motives were neither clearly left- nor right-wing. He had his first significant encounter with the health system after a serious back injury, and the experience seems to have radicalized him.
His crime is a classic example of “propaganda by the deed.” People who acknowledge intellectually that murder is wrong seem totally unemotional about that conclusion. There’s widespread support for the shooter, while the victim has been dehumanized and reduced to a symbolic avatar for the industry and its sins.
Almost everyone has some story of being abused by the modern health insurance system. It’s even worse for the self-employed, who pay out of pocket for insurance. After paying premiums for years, the injured find themselves in a Kafkaesque battle with their insurance company over coverage, copays, and approved care.
The False Promise of Obamacare
It was not supposed to be this way.
Obamacare was supposed to provide universal coverage and make health care more affordable. After all, the law was called the Affordable Care Act. When the Obama administration proposed the law in 2009, it made many promises to sell it to the public and Congress.
One of the more famous ones was that “if you like your doctor, you can keep him.” Another was that if you like your insurance, you can keep that too. Finally, we were told this law would make us all healthier, as uninsured people would no longer wait until health problems became catastrophic before seeking care, typically in the emergency room.
This was the signature initiative of the Obama presidency, and the law has done none of these things. Care has become significantly more expensive. The quality of care has also gone down, with out-of-pocket expenses rising because of higher deductibles and out-of-pocket limits. Doctors are frequently dropped from plans, leaving patients unable to maintain continuity of care with those whom they have come to trust.
The country has not gotten any healthier, in spite of the enormous amount of money changing hands. The complexity of Obamacare has also led to the proliferation of highly paid billing specialists, administrators, and other overhead, none of which contributes directly to better care, but all of it costs money.
That MF looked right into the camera and lied to us. It’s what Marxists do. I’ve seen in the UK, EU and Canada that socialized or Government run healthcare just means less quality, longer waits for worse coverage and care. Obama only lied to the believers in him. I knew almost everything he said was a lie
My wife’s dumbass relatives in Denmark can’t brag enough to me about their free healthcare, to which I say you pay 70% taxes, so it’s not free. They try to make America into Denmark and what sort of works for 5 million doesn’t translate to 330+ million. They don’t get it because they mostly want to trash the US. Plus, they are socialist and we’re not.
Well, here’s the facts. It doesn’t work, the doctors are crummy, you have to wait for months and you can’t sue for malpractice, which at least 4 of her relatives have received for healthcare and are now injured.
Now this story:
Advocates for “universal health care” love to use Finland as an example of a system that works. That is an absurd comparison. Finland has a culturally homogeneous population of 5.6 million; that is just over half the population of Los Angeles County (9.6 million).
Better examples are England and Canada.
England has government-funded “universal health care” in the form of the National Health Service. The population of England is around 57 million people. Wait times for nonemergency care average 14 to 18 weeks, and thousands of people have been waiting more than 18 months. As of June of this year, 7.5 million Brits were waiting for already scheduled procedures and surgeries requiring hospital stays, more than 300,000 of whom had been waiting for more than a year.
Keep in mind that these scheduled – and delayed – procedures include diagnostic tests and treatments for illnesses like cancer. Shortages of physicians and treatment facilities force cancer patients to wait weeks – or months – for radiation or chemotherapy.
These delays have life-and-death consequences. In 2009, British medical journal Lancet reported that 51.1% of British cancer patients were alive five years after their diagnosis. By contrast, 91.9% of American cancer patients were alive five years after their diagnosis.
England’s problems are not limited to cancer care. Last year, Bloomberg News published a report analyzing the NHS’s own data. The results were shocking. In most areas of England, medical care failed to meet government goals in things as basic as minimum wait times for an ambulance to arrive in an emergency (goal: 30 minutes; reality: up to three hours) or the availability of hospital beds.
In Canada – another country with “universal health care,” the situation is nearly as bad. Canada has a population of nearly 40 million. The average wait time for treatment in Canada for a condition requiring a specialist’s care is more than six months. But in some provinces and for some procedures – like orthopedic surgery or neurosurgery – the wait is closer to a year, or even longer. Canadians face long waits – six weeks to three months – even for simple but vital diagnostic procedures like MRIs, CT scans or ultrasounds.
By contrast, in the United States – a country with 330 million people – the average wait time for a nonemergency appointment with a specialist is only 26 days (a situation that medical journal STAT called “a public health crisis”). The median time between diagnosis of cancer and commencement of treatment is 27 days. The average wait time for an ambulance here is seven minutes.
Here’s an important segment of the social engineering component of the Affordable Care Act (ACA), passed under the Obama presidency:
The ACA provides a strong emphasis on preventive medicine and primary care through insurance reform, increased reimbursement for primary care providers, funding to educate these providers, and incentives to attract providers into primary care. The Nurse Practitioners (NPs) are especially well prepared to educate providers on the use of evidence-based preventive care and to assist the U.S. healthcare system in its transformation toward this model.
In other words, under the rubric of preventative medicine, millions of people who might not have gone to see a doctor prior to ACA are being encouraged to go. To meet the cost of those millions of new patients, new institutions like urgent care centers are springing up. Physicians’ Assistants (P.A.s) and Nurse Practitioners (N.P.s) are being used to treat these people as well as more serious cases. The medical schools do not turn out enough M.D.s to treat the 30 million people (new “patients”) who are being channeled into the American health care system. As my primary care doctor (an M.D.) told me, there is increasing pressure on him to have a practice of only very sick people. He frankly told me that he does not want the stress of treating only the very sick all day, every day.
So, in the post-ACA morass, we have too many people going to see M.D.s who don’t need an M.D. We have too many very sick people that have to wait a very long time to get an appointment with an M.D. And…we have increasing numbers of P.A.s and N.P.s supervising the care of very sick people. With millions of dollars pouring into the health care system from the federal government, it becomes a boon to hospital income to have less qualified personnel who need to be paid less than M.D.s. It’s a morass depicting itself as “needed reform.” From the Hippocratic Oath to do the least harm, the health care world has shifted to the “principle” see the most people and diminishing the quality of health care. There is a trade-off between the numbers served, which increases, and the quality of care and professionalism, which decreases.
Since 2010, our government has “given free money” to people. Yes, billions were siphoned off the top to people that don’t need it and were just dipping their hands in the till. There are plenty of cases documented. In the court of law, it’s called money laundering.
COVID Relief Program is the ‘Biggest Fraud in a Generation’
We’ve known about the fraud associated with the COVID relief program known as the Paycheck Protection Program (PPP):
Many who participated in what prosecutors are calling the largest fraud in U.S. history — the theft of hundreds of billions of dollars in taxpayer money intended to help those harmed by the coronavirus pandemic — couldn’t resist purchasing luxury automobiles. Also mansions, private jet flights and swanky vacations.
They came into their riches by participating in what experts say is the theft of as much as $80 billion — or about 10 percent — of the $800 billion handed out in a Covid relief plan known as the Paycheck Protection Program, or PPP. That’s on top of the $90 billion to $400 billion believed to have been stolen from the $900 billion Covid unemployment relief program — at least half taken by international fraudsters — as NBC News reported last year. And another $80 billion potentially pilfered from a separate Covid disaster relief program.
COVID Relief Program is the ‘Biggest Fraud in a Generation’
Like hitchhiking; it’s ass, grass or cash, no one rides for free. The bill is now due and it’s being paid at the grocery store and the gas pump. I’ll give it to you that the gas pump prices don’t have to happen, but the current administration is just giving us pain. It was half the price a year and a half ago and the ability to take it back to that prices is available still, if they wanted to do it.

I went to a hospital today to have a procedure done. When the nurse apologized for the quantity of paperwork, I casually mentioned that things might become more complicated with Obamacare.
I was not ready for the answer. Actually, being in a very socially liberal city and healthcare system, I thought I was going to hear support for the program. I instead was told how government has corrupted the system, made it worse for both Doctors and patients and other horror stories. I replied that the government has not helped healthcare in a long time to which the nurse responded that the decline of morals in our culture was the beginning of the problem. How correct this nurse was.
Next, I met with the Doctor to go over what the procedure was going to entail. I again mentioned whether the healthcare system was affecting his job. Again I received a surprise answer.
The doctor told me of his passion for his practice all of his life. He then told me that what is being done to us by Washington has him considering getting out. He was honorable enough to not practice if he couldn’t do his best. It was a John Galt conversation. There are others like this doctor. I’ve found that if you are contemplating your retirement in your mind, you are already in the process of retiring.
To a person, the hospital staff admitted that Washington and the damage they have done and are doing to our healthcare system makes it worse for patients and providers. This is not a partisan statement for the record.
Let me point out that this was a highly successful practice with state of the art equipment and professional personnel making these perspicacious comments to me.
It was clear that they wanted to help people and do their job, but our own government is in the way. It seems obvious that they have overstepped their role in making sure that medicine is safe and lawful.
If I hadn’t heard it from the horse’s mouth, I wouldn’t have known. I did go in looking for a cure, but I left with a dose of information. It is easy to conclude that we need to fix or excise Washington from the healthcare system and put it back in the hands of the doctors.
After 18 years in private practice, many good, some not, I am making a very big change. I am leaving my practice.
No, this isn’t my ironic way of saying that I am going to change the way I see my practice; I am really quitting my job. The stresses and pressures of our current health care system become heavier, and heavier, making it increasingly difficult to practice medicine in a way that I feel my patients deserve. The rebellious innovator (who adopted EMR 16 years ago) in me looked for “outside the box” solutions to my problem, and found one that I think is worth the risk. I will be starting a solo practice that does not file insurance, instead taking a monthly “subscription” fee, which gives patients access to me.
I must confess that there are still a lot of details I need to work out, and plan on sharing the process of working these details with colleagues, consultants, and most importantly, my future patients.
Here are my main frustrations with the health care system that drove me to this big change:
Here are some things that are not reasons for my big change:
What will my practice look like? Here are the cornerstones on which I hope to build a new kind of practice.
This is the first of a whole bunch of posts on this subject. My hope is that the dialog started by my big change (and those of other doctors) will have bigger effects on the whole health care scene. Even if it doesn’t, however, I plan on having a practice where I can take better care of my patients while not getting burned out in the process.
Is this scary? Heck yeah, it’s terrifying in many ways. But the relief to be changing from being a nail, constantly pounded by an unreasonable system, to a hammer is enormous.
From Kevin MD:
Three out of four dentists recommend this tooth brightening toothpaste — make your smile sparkle like never before! Six out of seven plumbers recommend this drain opening de-clogger — make your bathtub drain like never before! Nine out of ten doctors recommend improving the medical system in the United States — make your health care system heal like never before!
But how do we do that?
Do doctors think the Affordable Care Act is the soothing balm for the festering wound that is the economics of the American medical system—paying too much while delivering too little population health? What do our health care experts think about health care reform? Do we think it is a step in the right direction? A step towards doom and damnation? A small step for insurance companies, a huge leap for mankind?
It goes on to say that they need to read the bill to see what is in it.
However, here is what is in the bill click on it to find out what is in the bill and what rights we the people lose like financial control over our own assets and our own doctors. We do lose that despite what congress and the POTUS say to the contrary.
I checked in with KevinMD for this piece of helpful information. The free market will produce a better product than the government will ever be able to handle. Capitalism always provides competition which drives DOWN prices and drives UP services.
f you cannot measure it, you cannot improve it.
-Lord Kelvin
Asking science to explain life and vital matters is equivalent to asking a grammarian to explain poetry.
-Nassim Nicholas Taleb
Of course the quantified self movement with its self-tracking, body hacking, and data-driven life started in San Francisco when Gary Wolf started the Quantified Self blog in 2007. By 2012, there were regular meetings in 50 cities and a European and American conference. Most of us do not keep track of our moods, our blood pressure, how many drinks we have, or our sleep patterns every day. Most of us probably prefer the Taleb to the Lord Kelvin quotation when it comes to living our daily lives. And yet there are an increasing number of early adopters who are dedicated members of the quantified self movement.
They are an eclectic mix of early adopters, fitness freaks, technology evangelists, personal-development junkies, hackers, and patients suffering from a wide variety of health problems. What they share is a belief that gathering and analysing data about their everyday activities can help them improve their lives.
According to Wolf four technologic advances made the quantified self movement possible:
First, electronic sensors got smaller and better. Second, people started carrying powerful computing devices, typically disguised as mobile phones. Third, social media made it seem normal to share everything. And fourth, we began to get an inkling of the rise of a global superintelligence known as the cloud.
An investment banker who had trouble falling asleep worried that his concentration level at work was suffering. Using a headband manufactured by Zeo, he monitored his sleep quantity and quality, and he also recorded data about his diet, supplements, exercise, and alcohol consumption. By adjusting his alcohol intake and taking magnesium supplements, he has increased his sleeping by an hour and a half from the start of the experiment.
A California teacher used CureTogether, an online health website, to study her insomnia and found that tryptophan improved both her sleep and concentration. As an experiment, she stopped the tryptophan and continued to sleep well, but her ability to concentrate suffered. The teacher discovered a way to increase her concentration while curing her insomnia. Her experience illustrates a phenomenon that Wolf has noticed: “For many self-trackers, the goal is unknown … they believe their numbers hold secrets that they can’t afford to ignore, including answers to questions they have not yet thought to ask.”
Employers are becoming interested in this approach in connection with their company sponsored wellness programs. Suggested experiments include using the Jawbone UP wristband to see if different amounts of sleep affect work performance such as sales or using the HeartMath emWave2 to monitor pulse rates for determining what parts of the workday are most stressful.
Stephen Wolfram recently wrote a blog illustrating just how extensive these personal analytics experiments in self-awareness could become when coupled with sophisticated technologies. Wolfram shares graphs of his “third of a million emails I’ve sent since 1989” and his more than 100 million keystrokes he has typed.
Anyone interested in understanding just how far reaching this approach may become in the future should examine the 23 pages of projects being conducted by the MIT Media Center. My favorites from this fascinating list include automatic stress recognition in real-life settings where call center employees were monitored for one week of their regular work; an emotional-social intelligence toolkit to help autism patients learn about nonverbal communication in a natural, social context by wearing affective technologies; and mobile health interventions for drug addiction and PTSD where wearable, wireless biosensors detect specific physiological states and then perform automatic interventions in the form of text/images plus sound files and social networking elements.
It is easy to get caught up in the excitement of all this new technology and to start crafting sentences about how the quantified self movement will “transform” and “revolutionize” health care and spawn wildly successful new technology companies.
Jackie Fenn’s “hype cycle” concept has identified the common pattern of enthusiasm for a new technology that leads to the Peak of Inflated Expectations, disappointment that results in the Trough of Disillusionment and gradual success over time that concludes in the Slope of Enlightenment and the Plateau of Productivity. Fenn’s book, Mastering the Hype Cycle: How to Choose the Right Innovation at the Right Time can help all of us realize that not all new technologies becomes killer applications.
Jay Parkinson, MD has also written a blog that made me pause before rushing out to invest in quantified self companies or predict the widespread adoption of this approach by all patients. Parkinson divides patients into three groups. The first group is the young, active person who defines health as “not having to think about it until they get sick or hurt themselves.” The second group is the newly diagnosed patient with a chronic illness that will affect the rest of their lives. After a six month period of time coming to terms with their illness, Parkinson believes this group moves closer and closer to group one who do not have to think about their disease. The third group are the chronically ill who have to think about their disability every day. Parkinson concludes that “it’s almost impossible to build a viable social media business that focuses on health. It’s the wrong tool for the problem at hand.”
The quantified self movement should be closely monitored by all interested in the future of the American health care delivery system. The potential to improve the life of patients with chronic diseases is clearly apparent; whether most people will use the increasingly sophisticated tools being developed is open to debate.
From the Raleigh WRAL sometimes news.
WASHINGTON — Death, taxes and now health insurance? Having a medical plan or else paying a fine is about to become another certainty of American life, unless the Supreme Court says no.
People are split over the wisdom of President Barack Obama’s health care overhaul, but they are nearly united against its requirement that everybody have insurance. The mandate is intensely unpopular even though more than 8 in 10 people in the United States already are covered by workplace plans or government programs such as Medicare. When the insurance obligation kicks in, not even two years from now, most people won’t need to worry or buy anything new.
Nonetheless, Americans don’t like being told how to spend their money, not even if it would help solve the problem of the nation’s more than 50 million uninsured.
Can the government really tell us what to buy?
Federal judges have come down on both sides of the question, leaving it to the Supreme Court to sort out. The justices are allotting an unusually long period, six hours over three days, in sessions that started Monday, to hear arguments challenging the law’s constitutionality.
Their ruling, expected in June, is shaping up as a historic moment in the century-long quest by reformers to provide affordable health care for all.
Many critics and supporters alike see the insurance requirement as the linchpin of Obama’s health care law: Take away the mandate and the wheels fall off.
Politically it was a wobbly construction from the start. It seems half of Washington has flip-flopped over mandating insurance.
One critic dismissed the idea this way: “If things were that easy, I could mandate everybody to buy a house and that would solve the problem of homelessness.” That was Obama as a presidential candidate, who was against health insurance mandates before he was for them.
Once elected, Obama decided a mandate could work as part of a plan that helps keep premiums down and assists those who can’t afford them.
To hear Republicans rail against this attack on personal freedom, you’d never know the idea came from them.
Its model was a Massachusetts law signed