Yes, and it stopped Covid also, but do you think they bothered telling anyone that?
Evidence continues to accumulate showing that vitamin D is a strong ally to combat cancer
Low vitamin D levels are linked to an increased risk of cancers, while vitamin D can attach to the vitamin D receptor (VDR) in your cells, setting off a series of signals that may affect how they grow, develop and survive
Although increasing vitamin D levels may help to reduce cancer deaths, health officials rarely recommend optimizing levels for this purpose
Vitamin D targets cancer in multiple ways, including anticancer, antimetastatic and anti-tumorigenic effects
The best way to optimize your vitamin D level is via regular sun exposure, which enhances production of melatonin — a potent anticancer agent
(Mercola)—I strongly recommend getting sensible sun exposure each day, and one of the reasons why is because it helps naturally optimize your vitamin D levels. Low vitamin D levels are linked to an increased risk of cancers,1 while vitamin D can attach to the vitamin D receptor (VDR) in your cells, setting off a series of signals that may affect how they grow, develop and survive.2
The use of ivermectin to treat COVID-19 is an ongoing debate. The central conflict is that while many doctors have reported success in using ivermectin, some studies published in major journals suggest it is in fact ineffective.
(eloresnorwood/Shutterstock)
Even as the FDA recently has been removing misinformation it posted about ivermectin, the agency has maintained its original position regarding its effectiveness, namely that there isn’t evidence.
People who trust ivermectin claim the studies showing ineffectiveness are fraudulent, while people who are skeptical of its use for treating COVID-19 view it as an anti-science conspiracy theory.
As a professional with decades of research experience conducting dozens of clinical trials on antiviral drugs, I decided to dive deep into the studies purporting ivermectin’s ineffectiveness. What I found shocked me.
Legacy Media Report Ineffectiveness
Numerous preclinical studies have found that ivermectin has a broad range of effects on COVID-19, spanning from its initial impact on viral infection to the pathological changes the virus causes in our bodies.
Ivermectin inhibits the entire life cycle of SARS-CoV-2 in our cells from attachment, spreading, and replication (1, 2, 3).
Ivermectin exceeds the approved antiviral effects of other medications, including Paxlovid, molnupiravir and remdesivir, which only target the virus and lack anti-inflammatory and organ-protective effects. Monoclonal antibodies have to be constructed specific to each variant and are very expensive.
Let’s take a trip down memory lane, all the way back to the ancient times of early 2021, to see how “the science” on mRNA Covid-19 shots has evolved in such a short period of time.
1) It’s the cure!
In the words of former CDC Director Rochelle Walensky: “Vaccinated people do not carry the virus and don’t get sick.”
Let’s take a trip down memory lane, all the way back to the ancient times of early 2021, to see how “the science” on mRNA Covid-19 shots has evolved in such a short period of time.
2) It’s not the cure but it prevents you from getting it and spreading it to others
In the words of The Science himself, the vaccine prevents Covid-19 from mutating. Hooray science!
Let’s take a trip down memory lane, all the way back to the ancient times of early 2021, to see how “the science” on mRNA Covid-19 shots has evolved in such a short period of time.
In the words of The Science himself, the vaccine prevents Covid-19 from mutating. Hooray science!
3) It doesn’t prevent you from getting it but it prevents you from getting sick
Okay, so in the UPDATED words of The Science himself, “the situation is so clear, the data affirm, if you get the vaccinated you are protected … we know that as a fact.”
4-9 at the link below
10) Okay, it’s poison, and it doesn’t actually do anything beneficial whatsoever. There are no benefits, only costs. The cure is so much worse than the disease. We got bamboozled every step of the way
More questions are being raised about Dr Anthony Fauci‘s ties to the Covid lab leak theory after the release of a tranche of new emails.
The former White House advisor, 83, was hit with a series of new allegations this week including that he secretly conspired with the CIA to squash debate about the origins of the virus.
Leaked documents also showed that Dr Fauci’s top aide intentionally tried to hide his discussions about the virus’s genesis by using his personal email.
And now new messages show Dr Fauci was engaged in some form of ‘damage control’ at the time his department was being probed about funding to the Chinese laboratory feared to have started the pandemic.
The April 2020 email, sent between Dr Fauci’s aide and a third-party group who distributed government grants to China, suggests they were concerned about backlash coming from the probe.
EcoHealth Alliance, headed by Dr Peter Daszak, helped fund research at the Wuhan lab using grants from Dr Fauci’s department, the National Institute of Allergy and Infectious Disease (NIAID).
The lab had enjoyed part of a $3.3 million in US taxpayer funds since 2014 to conduct experiments on bat coronaviruses.
At the end of 2019, the virus that would eventually spark a global pandemic emerged in Wuhan with early cases linked to a seafood market just eight miles away from the lab.
In April 2020, when 787,000 Americans had gotten sick and 42,000 had died of Covid, EcoHealth hit a regulatory snag.
Senator Rand Paul (R-KY), a US Senator and Doctor of Ophthalmology, released a stunning report on Tuesday where he discovered that 15 different federal agencies knew that the Wuhan laboratory in China was trying to create a COVID-19 virus and they knew this since 2018.
Not one single official or employee in these 15 agencies revealed the truth to the American public during the pandemic. They should all be fired.
In 2019 the virus escaped from the Wuhan laboratory at the same time US President Donald Trump had crippled the Chinese economy with his economic policies. The rest is history.
Dr. Tony Fauci, who funded the Wuhan laboratory for some reason, repeatedly lied to the American public about the origins of the virus.
As The Gateway Pundit reported back in May 2023, Fauci gave a $1.88 million grant and $16.5 million in NIH funding to a British scientist in January 2020 if he kept his mouth shut about the origins of the COVID-19 virus.
On January 31, 2020, Danish-born and British-educated scientist Kristian Andersen, emailed Dr. Tony Fauci saying the virus looks lab-made.
Kristian Anderson, “Some of the features look engineered” and the “genome looks inconsistent with evolutionary theory.”
What the CDC recently reported (see chart below), however, is that by the end of 2023, cumulatively, at least 87% of Americans had anti-nucleocapsid antibodies to and thus had been infected with SARS-CoV-2, this in spite of the mammoth, protracted and booster-repeated vaccination campaign that led to about 90% of Americans taking the shots. My argument is that by making policies based on number of infections a higher priority than ones based on the more serious but less common consequences of both infections and policy damages, the proclaimed goal of the vaccine mandate to reduce spread failed in that 87% of Americans eventually became infected anyway.
In so many words—and data—CDC has quietly admitted that all of the indignities of the Covid-19 pandemic management have failed: the masks, the distancing, the lockdowns, the closures, and especially the vaccines; all of it failed to control the pandemic.
It’s not like we didn’t know that all this was going to fail, because we said so as events unfolded early on in 2020, that the public health management of this respiratory virus was almost completely opposite to principles that had been well established through the influenza period, in 2006. The spread of a new virus with replication factor R0 of about 3, with more than one million cases across the country by April 2020, with no potentially virus-sterilizing vaccine in sight for at least several months, almost certainly made this infection eventually endemic and universal.
Covid-19 starts as an annoying, intense, uncomfortable flu-like illness, and for most people, ends uneventfully 2-3 weeks later. Thus, management of the Covid-19 pandemic should not have relied upon counts of cases or infections, but on numbers of deaths, numbers of people hospitalized or with serious long-term outcomes of the infection, and of serious health, economic, and psychological damages caused by the actions and policies made in response to the pandemic, in that order of decreasing priorities.
Even though numbers of Covid cases correlate with these severe manifestations, that is not a justification for case numbers to be used as the actionable measure, because Covid-19 infection mortality is estimated to range below 0.1% in the mean across all ages, and post-infection immunity provides a public good in protecting people from severe reinfection outcomes for the great majority who do not get serious “long-Covid” on first infection.
Actions have consequences. For the sheep who fell for it and got jabbed, the bill is coming due. You won’t read a thing about the Covid Jab in the article below, but it’s as obvious as your face in the mirror. They blame it on everything but the reason.
ounger generations are aging more rapidly, and this could be leading to an increased risk of cancer, a new study says.
People born in or after 1965 are 17% more likely to be experiencing accelerated aging compared to seniors born between 1950 and 1954, researchers found.
That faster aging is associated with a higher risk of certain cancers among adults younger than 55, also known as early-onset cancers, results show.
“Multiple cancer types are becoming increasingly common among younger adults in the United States and globally,” researcher Ruiyi Tian, a doctoral student at Washington University School of Medicine in St. Louis, said in a news release. “Understanding the factors driving this increase will be key to improve the prevention or early detection of cancers in younger and future generations.”
For this study, researchers analyzed blood data for nearly 149,000 people participating in the U.K. Biobank project.
The team used a set of nine biomarkers found in blood to calculate each person’s biological age, or what age a person appears to be based on the condition of their body.
They then contrasted that to the person’s actual age based on their birth date, as well as any cancers that had occurred among them.
This is in response to the FDA’s infamous tweet: “You are not a horse. You are not a cow. Serious y’all. Stop It.”
Other facts the FDA ignored:
Ivermectin has one of the best safety profiles in all of medicine.
Its discovery won the Nobel Prize.
Doctors are allowed to use medications off-label, especially when they are shown to be effective.
102 studies from 1,139 scientists show ivermectin’s effectiveness in treating COVID-19.
Ivermectin is often recognized—as second only to penicillin—for having one of the greatest impacts on human health, particularly for its role in bringing river blindness to the brink of extinction.
Ivermectin, frequently hailed as a “wonder drug,” is now emerging as a potentially “powerful drug” for fighting cancer.
A world-leading virologist has issued a shocking warning to the American public that a “massive tsunami” of death will soon destroy the global COVID-19 vaccinated population.
As Slay News reported, the bone-chilling warning was issued by Dr. Geert Vanden Bossche, a respected Belgian virologist, during an appearance on the KunstlerCast podcast, which is hosted by James Kunstler, on Friday.
Dr. Bossche is certified in both Virology and Microbiology and is the inventor of a patent application for universal vaccines. He has also authored over 30 publications and currently works as an independent research consultant.
Dr. Bossche, however, is most famous for warning about the potential dangers of mass vaccination programs amid the COVID-19 pandemic. He warned that the programs could lead to “monster” COVID variants.
The virologist told Kunstler that shortly, a “massive tsunami” of death among the vaccinated would happen. This would start with far more cases of long COVID, which would replace the surge of cancers, and end with a “hyper-acute wave.”
“What I am predicting is a massive, massive tsunami of illness and death among highly vaccinated populations with compromised immune systems, Bossche said. “You will see what will happen, for example, in the next coming week is more and more cases of more serious long Covid.”
“They will start to replace the surge of the cancers,” he continued. “It will end with a hyper-acute phase, a huge, huge wave.”
More than a quarter of participants in a study from Saudi Arabia reported cardiac complications after receiving mRNA COVID-19 vaccines, and many of them required hospitalization or intensive care.
The onset of cardiac complications varied among participants, with 14.55% experiencing symptoms within one month of vaccination and others reporting issues up to 12 months or longer.
TrialSite News reported on the “bombshell Saudi Arabian study” on Wednesday. Founder, Daniel O’Connor, told The Defender that while the study has limitations and was designed to look for cardiac complications, “The rate of hospitalized cases was certainly notable, especially given the existing cardiac (myocarditis/pericarditis) signal associated with the vaccines.”
If someone wished to destroy America, could he do anything more catastrophic than what we currently see and hear each day? What would an existential enemy do that we have not already done to ourselves?
Here are eleven now familiar steps to civilizational destruction:
1) Wipe out a 2,000 mile border. Allow 10-million foreign nationals to enter unlawfully. Have no audit of any; nullify all federal immigration laws. Let toxic drugs in that kill 100,000 Americans a year. Give free support for those millions who broke the law. Smear any objectors as racists and xenophobes.
2) Run up $35 trillion in national debt. Keep adding $1 trillion to it each 100 days. Defame anyone wishing to cut wild spending as cruel and inhumane.
AP Award-Winning Photograph of murdered rape victim beingtransported to Gaza for purposes of necrophilia.
3). Appease or subsidize enemies like Iran and China. Demonize allies like Israel. Allow terrorists to attack Americans without response. See Islam as either similar or superior to Christianity. Make amends to leftist governments for supposedly past toxic American international behavior. Follow the lead of international agencies like the UN, ICC, and WHO to atone forpast American neocolonial and imperialist behavior. Recede to second-tier international status, befitting American decline.
4) In a multiracial democracy, redefine identity only as one’s tribal affiliation. Ensure each identity group rivals the other for victimhood and the state spoils it confers. Redefine all political issues by race and sex oppressors and oppressed. Destroy all meritocratic standards of admission, retention, promotion, and commendation.
5) Redefine violent crime as understandable, cry-of-the-heart expressions of social justice. Ensure no bail and same-day release for arrested, repeat violent felons. Empathize with the violent killer and rapist; ignore their victims, especially if slain police-officers.
6). Emasculate the military by using non-meritocratic standards of race, gender, and sexual orientation to determine promotion and commendation. Deliberately smear as racists and insurrectionists the largest demographic in the military who in recent wars died at twice their numbers in the population—so that they leave or never join the military. Encourage retired high officers to slander their Commander-in-Chief. Cut the defense budget. Stop producing sufficient weapons, but leave billions of dollars’ worth of arms to terrorists.
7) Reinvent the justice system to indict, bankrupt, convict, jail and eliminate political opponents. Use ballot removal, impeachment, civil suits, and state and federal indictments rather than elections to defeat an opponent. Mob the homes of non-compliant Supreme Court Justices, attack them personally by name.
8) Encourage the fusion of the bureaucratic state with the electric media to form a powerful force for political audit, surveillance, censorship, and coercion. Marry the FBI to Silicon Valley and hire its contractors to warp the news and hound supposed enemies of the people.
9.) Make war on affordable gasoline and natural gas. Substitute inefficient, unreliable, and expensive wind and solar power, even as energy prices bankrupt the middle class.
10.) Marry late, but preferably not at all. Consider males toxic, especially boys. Have no children, or as few as possible. Otherwise, assure children they are entitled, and must be sheltered. Raise them to have grievances against past generations and current norms.
11.) Turn world-class universities into indoctrination centers. Suspend the Bill of Rights on campuses. Train youth to graduate despising their own culture and civilization. Recruit foreign students from hostile nations to subsidize campus commissarbloat. Replace the curriculum with therapeutic propaganda. Ban the SAT/ACT and do not evaluate high school GPAs. Ensure merit does not select the student body. Charge tuition higher than the rate of inflation. Bill the government when students default on their loans.
So why are those controlling Biden using him to advance much of such a destructive agenda that would end America as we know it?
1) They are delusional and think their socialist and globalist agendas are working and will save us.
2) They are raging nihilists who do not like the U.S. and deliberately want it destroyed as a service to the world. A ruined U.S. is preferable to a strong America.
3) They are Jacobin revolutionaries who are intentionally erasing the old United States as a prerequisite for creating an entirely new America that will arise from the ashes with no trace or even memory of its past.
4) They have no agenda. They are aimless fools, and utter incompetents. These bunglers just wing it day-to-day, in response to what their radical media, academic, and political masters dictate is necessary for them to retain power. They have no idea of the damage they are doing.
Vaccine Lettuce — that’s what Tennessee calls the food if it has antibody-producing material added to it.
Governor Bill Lee is expected to sign into law a bill aimed at classifying as “drugs” any food that contains vaccine material.
The legislation, HB 1894, passed the House early last month in a 73-22 vote, and last Thursday, the Senate approved it by an equally high margin of 23-6. The bill defines “vaccine material” as any substance intended “for use in humans to stimulate the production of antibodies and provide immunity against disease.”
Tennessee does not intend to ban the sale of vaccine-laced foods, but it does want to require that they are labeled properly and that people obtain a prescription from a doctor prior to consuming them.
A United States Navy medic who blew the whistle on an explosive report showing a massive increase in heart issues among military pilots has been blocked by the Department of Defense (DOD) from accessing his work computer. Navy Medical Service Corps Lt. Ted Macie shared shocking information about the surge in heart failure among military personnel. Macie claimed that members of the U.S. military have experienced massive increases in heart-related issues, presenting Defense Department data showing the following.
937% increase in heart failure
· 152% increase in cardiomyopathy
· 69% increase in ischemic heart disease
· 36% increase in hypertensive disease
· 63% increase in other forms of heart disease
According to information published by the U.S. Army, 97% of active-duty U.S. troops are fully vaccinated, 90% of Army National Guard members are fully vaccinated, and 91% of U.S. Army Reserve members are fully vaccinated.
I have tried to avoid the jab, mRNA, and all of the other poison they tried to stab us with. Now, they are giving mRNA shots to pigs and cows to get it to humans through food.
Here’s the lie…..
The big question in the industry was whether vaccinations could replace antibiotics. The problem was specificity to disease and long development horizons. Then came the breakthrough: mRNA. About 12 years ago the poultry industry began using mRNA. About 5 years ago the pork industry joined and about 2 years ago cattle followed.
Have you noticed the “antibiotic free” messaging from the industry lately? They don’t say “substitute mRNA for antibiotics.” They just say “antibiotic free.” This is one of the most clever-speaks ever invented.
Of course, just like rBGH in dairy cows—remember that?—used for nearly a decade before going on the label—mRNA has been used for some time without widespread knowledge. Dr. Joe Mercola discovered this in the spring of 2023 and alerted Americans that it was already in our meat. I was unaware of it, like almost everyone else.
Since then, the industry has circled the wagons. When testimony in Missouri’s legislature revealed its use in cattle, the industry quickly put out a press release stating mRNA was “not licensed” for use in cattle. This is a common sleight of words. The industry did not say “We aren’t using it;” notice the words: “not licensed.” The obvious inference to the average consumer is that it’s not being used.
But all sorts of exemptions and loopholes exist around drugs. Both experimental and emergency use make an end run around licensing. This was the case with rBGH in dairy cows. The dairy industry didn’t have to disclose its use, on labels or otherwise, due to its “experimental” designation. If you’re thinking what I’m thinking (Pinky and the Brain) this sounds extremely similar to the clever-speak surrounding mRNA use on humans during Covid—experimental and emergency.
Top doctors are warning of an “epidemic” of cancers normally seen in older people that are now affecting younger, fit, healthy people and are unsure of the cause.
After the Princess of Wales announced on Friday that she was being treated for cancer, specialist clinicians said they were seeing much larger numbers of “fit and outwardly healthy” under 45’s presenting with cancers than ever before.
“One study that looked at data from Northern Ireland between 1993 and 2019 found the rate of early-onset cancers increased by 20.5 per cent, the equivalent of about 7,000 extra cases a year across the UK,” reports the Telegraph.
Health experts are baffled as to what is causing the new trend, which is primarily centered on the abdominal area.
“When I started as a cancer surgeon 20 years ago, you rarely saw any younger patients, but now I see them regularly,” said Prof Andrew Beggs, a consultant colorectal surgeon and a senior clinical fellow at the University of Birmingham.
WCW has uncovered an alarming pattern of recent animal lab accidents at Colorado State University, which is working with the notorious EcoHealth Alliance and the NIH to build a new bat lab and breeding colony.
Never-before-seen records obtained by WCW show that from 2020 to 2023, dozens of animal lab accidents with bats, cats, hamsters, and mice exposed CSU staff to coronaviruses, Zika, rabies, Tuberculosis, and other dangerous pathogens that can cause deadly outbreaks.
Last year, WCW exposed how $12 million of taxpayers’ money is being wasted by CSU and EcoHealth to build a new lab and import hundreds of bats from Asia to establish a new breeding colony and infect them with deadly viruses, including Ebola and Nipah
The new bat lab at CSU is now scheduled to be completed in December 2024
Last year, White Coat Waste Project (WCW) exposed how $12 million of taxpayers’ money is being wasted by Colorado State University (CSU) and Wuhan lab partner EcoHealth Alliance (EHA) to build a new lab at CSU and import hundreds of bats from Asia to establish a new breeding colony and infect them with deadly viruses, including COVID, Ebola and Nipah.
On October 5, 2015, Nature reported, “Three scientists who developed therapies against parasitic infections have won this year’s Nobel Prize in Physiology or Medicine.
“The winners are: William C. Campbell, a microbiologist at Drew University in Madison, New Jersey; Satoshi Ōmura, a microbiologist at Kitasato University in Japan; and Youyou Tu, a pharmacologist at the China Academy of Chinese Medical Sciences in Beijing.
“In the 1970s, Campbell and Ōmura discovered a class of compounds, called avermectins, that kill parasitic roundworms that cause infections such as river blindness and lymphatic filariasis. The most potent of these was released onto the market in 1981 as the drug ivermectin.”
Six years later, our Banana Republic government, led by Biden the Bribed, mocked ivermectin — dismissing it as horse paste. The reason, an off-the-shelf remedy for covid would have demoted Operation Warp Speed to Operation Follow the Law and FDA Rules.
Ivermectin worked, so the FDA tweeted, “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
Y’all.
To the elitists in DC (none of whom are actually elite at anything worthwhile) the people they are supposed to serve are rubes. The tweet promoted an unsigned FDA press release, “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
The piece said, “There seems to be a growing interest in a drug called ivermectin for the prevention or treatment of COVID-19 in humans. Certain animal formulations of ivermectin such as pour-on, injectable, paste, and ‘drench,’ are approved in the U.S. to treat or prevent parasites in animals. For humans, ivermectin tablets are approved at very specific doses to treat some parasitic worms, and there are topical (on the skin) formulations for head lice and skin conditions like rosacea.”
Horse paste.
The FDA promoted on late-night TV its disinformation campaign against using a Nobel-winning wonder drug against covid.
The Week reported, “Late night hosts are baffled anyone chooses horse de-wormer over COVID-19 vaccines.”
I am not baffled as to why all the late-night hosts simultaneously decided to mock ivermectin because if I learned anything from the Twitter files it is that the government bureaucracy will use your money to pay off corporate media to carry its message and to censor you.
The propaganda piece said, “The FDA has not authorized or approved ivermectin for the treatment or prevention of COVID-19 in people or animals. Ivermectin has not been shown to be safe or effective for these indications.”
The same could be said for what the FDA passed along as vaccines. The FDA may have approved them on an emergency basis, but they had not been shown to be safe or effective for” covid. Since then, we know there is no covid vaccine. There was a covid shot, of course, which mitigated the damage from the virus but it was not a vaccine in that it neither protected the patient from the virus nor did it stop the spread of covid.
The covid shot was like a flu shot. I don’t get them, but my wife did when she was still mobile. To each his (or her) own. I got the covid shot in deference to her because I would never hear the end of it if I killed her. We will spend eternity together, so I am cleaning up my act.
The FDA is, too.
Emily Miller reported on Friday, “The Food and Drug Administration settled the lawsuit brought by three doctors who use ivermectin off-label to treat COVID-19. The FDA agreed to delete social media posts opposing the medication by saying it is for horses.
“Dr. Mary Talley Bowden of Day 8, the plaintiff in the case, told me: ‘The damage the FDA inflicted will linger, but future patients are now protected from one meaningful government intrusion into their medical care.’”
This is locking the medicine cabinet door long after the horse paste hoax had escaped. We do not know how many lives could have been saved if the FDA did not throw shade on ivermectin.
Then again, we don’t know how many people died from covid. Oh, we know how many people died WITH covid. If you had covid and died in a car accident, you counted as a person who died WITH covid. Lucky you.
But how many people covid actually killed will never be known and for good reason. The government did not want you to know. The government thrives in an emergency. Ginning up the numbers kept that emergency going.
I am not an anti-vaxxer. I am very pro-vaccine. Vaccines are a miracle that have eradicated smallpox, which killed one-third of the people who contracted it. The polio vaccine meant kids could be free to go swimming again.
Sure I had measles, chicken pox, German measles and mumps as a kid. I survived. But I gladly would like back the 8 weeks that I spent recovering from the 4. The MMR shot is a miracle. Childhood diseases have a low mortality rate (the odds of dying from measles is at about 1 in 1,000) but why have them at all? Inoculate! There is no link between autism and MMR. The Lancet medical journal lied.
What makes such a lie dangerous is now no one believes what the Lancet published before. That is an awful loss of scientific papers. Surely, not every paper it published was a lie but now none can be trusted.
The FDA has joined the Lancet when it comes to credibility, and that puts everyone in harm’s way because we no longer have someone to turn to for making sure our foods and drugs are safe. The damage done by covid is more than just a wrecked economy that DC is trying to save by foolishly borrowing another trillion dollars every 100 days.
For you see, the boy who cried wolf eventually did indeed face a wolf and no one came to his rescue.
And someday, the federal bureaucracy that cried horse paste will someday face real danger and no one will believe it.
That 2015 article in Nature said, “This year’s prize highlights the global acceptance of the importance of parasitic infections, and neglected tropical diseases in general, says Stephen Ward at the Liverpool School of Tropical Medicine, UK. He notes that artemisinin has ‘saved possibly millions of lives’ — although resistance to the drug is on the rise in parts of southeast Asia — and that ivermectin has protected millions from disease.”
Thanks to our government, it saved only dozens of people from covid in the USA.
Last week, the Robert Koch Institut (the German CDC) released over 2,500 pages documenting the meetings of the “Covid Crisis Team” between January 2020 and April 2021. They did so in response to long-running litigation by journalists at Multipolar.
This is a major revelation – a rough German equivalent of the Fauci email releases from 2021 – which takes us directly into the internal discussions of the pandemic managers throughout the 2020 lockdowns and the early stages of the vaccination campaign. You can download the minutes and agendas yourself here. They’re heavily redacted, but they provide a dismal view of the whole pandemic circus and its idiotic, hapless coordinators. It will take me weeks to finish studying them, but German Twitter has done the Lord’s work unearthing many of the more important revelations, as does this surprisingly critical ZDF article. Here I want to highlight just three points.
The spike protein, which is the antigen of SARS-CoV-2 and genetic vaccines, has already been found to have various toxicities, including effects on red blood cells and platelet aggregation, amyloid formation, and neurotoxicity. It is essential to recognise that the spike protein itself is toxic to humans. It has also been reported that the spike protein can cross the blood–brain barrier. Therefore, it is essential to remove the spike protein derived from the gene vaccine itself from blood products.
2.Contamination with amyloid aggregates and microthrombi formed by spike proteins
It is not yet clear how the amyloid aggregates and microthrombi formed by the spike proteins develop into visible thrombi. However, once formed, amyloid aggregates may not be readily cleared and therefore need to be removed from blood products. These amyloid aggregates have also been shown to be toxic.
3. Events attributable to decreased donor immune system and immune abnormalities due to immune imprinting or class switch to IgG4, etc. resulting from multiple doses of genetic vaccines
When the immune function of a donor is impaired by gene vaccination, there is a risk that the donor has some (subclinical) infectious disease or is infected with a pathogenic virus and has developed viremia or other conditions, even if the donor has no subjective symptoms. For this reason, healthcare professionals who perform surgical procedures, including blood sampling and organ transplantation, as well as using blood products, should manage the blood of genetic vaccine recipients with care to prevent infection through blood. It will also be necessary to inform all healthcare professionals of these risks.
4. Lipid nanoparticles (“LNPs”) and pseudouridinated mRNA (mRNA vaccines only)
In the case of mRNA vaccines, LNPs and pseudouridinated mRNA may remain in the blood of recipients if blood is collected without a sufficient deferral period after gene vaccination. LNPs are highly inflammatory and have been found to be thrombogenic themselves, posing a risk to transfusion recipients. LNPs themselves have potent adjuvant activity and are at risk of inducing Adjuvant-Induced Autoimmune Syndrome (“ASIA syndrome”). An additional risk is that if the pseudouridinated mRNA is incorporated into the recipient’s blood while still packaged in LNPs, additional spike protein may be produced in the recipient’s body.
5. Contamination with aggregated red blood cells or platelets
The spike protein causes red blood cells and platelets to aggregate and therefore these aggregates will be carried into the recipient’s blood unless they are removed from the blood product.
6.Memory B cells producing IgG4 and IgG4 produced from them
Large amounts (serum concentration typically above 1.25–1.4 g/L) of non-inflammatory IgG4-positive plasma cells can cause chronic inflammation such as fibroinflammatory disease.
IgG4 is an antibody and is the acronym for immunoglobulin G4. Earlier in the paper, the authors wrote that “long-term exposure to a specific identical antigen (in this case, spike protein) causes immunoglobulins to become IgG4 and some of the B cells
that produce them are likely to differentiate into memory B cells that survive in the body for a sustained period, the immune dysfunction of genetic vaccine recipients is expected to be prolonged (Table 1, point 3 & 6). More details on these points are expected to be revealed in the future.”
(The Epoch Times)—Receiving blood transfusion from COVID-19-vaccinated individuals could pose a medical risk to unvaccinated recipients since numerous adverse events are being reported among vaccinated people worldwide, according to a recent study from Japan.
The preprint review, published on March 15, examined whether receiving blood from COVID-19-vaccinated individuals is safe or poses a health risk. Many nations have reported that mRNA vaccine usage has resulted in “post-vaccination thrombosis and subsequent cardiovascular damage, as well as a wide variety of diseases involving all organs and systems, including the nervous system,” it said.
Repeated vaccinations can make people more vulnerable to COVID-19, it said. If the blood contains spike proteins, it becomes necessary to remove these proteins prior to administration, and there is no such technology currently available, the authors wrote.
Contrary to earlier expectations, genes and proteins from genetic vaccines have been found to persist in the blood of vaccine recipients for “prolonged periods of time.”
In addition, “a variety of adverse events resulting from genetic vaccines are now being reported worldwide.” This includes a wide range of diseases related to blood and blood vessels.
Some studies have reported that the spike protein in the mRNA vaccines is neurotoxic and capable of crossing the blood-brain barrier, the review stated. “Thus, there is no longer any doubt that the spike protein used as an antigen in genetic vaccines is itself toxic.”
Moreover, people who have taken multiple shots of mRNA vaccines can have several exposures to the same antigen within a small time frame, which may lead to them being “imprinted with a preferential immune response to that antigen.”
This has resulted in COVID-19 vaccine recipients becoming “more susceptible to contracting COVID-19.”
Given such concerns, medical professionals should be aware of the “various risks associated with blood transfusions using blood products derived from people who have suffered from long COVID and from genetic vaccine recipients, including those who have received mRNA vaccines.”
The impact of such genetic vaccines on blood products as well as the actual damage caused by them are currently unknown, the authors wrote.
“In order to avoid these risks and prevent further expansion of blood contamination and complication of the situation, we strongly request that the vaccination campaign using genetic vaccines be suspended and that a harm–benefit assessment be carried out as early as possible.”
Repeated vaccination of genetic vaccines can also end up causing “alterations in immune function” among recipients. This raises the risk of serious illnesses due to opportunistic infections or pathogenic viruses, which would not have been an issue if the immune system were normal, the review said.
In December 2021, the FDA warned Americans not to use Ivermectin, which “is intended for animals” to treat or prevent COVID-19.
“Never use medications intended for animals on yourself or other people. Animal ivermectin products are very different from those approved for humans. Use of animal ivermectin for the prevention or treatment of COVID-19 in humans is dangerous,” FDA said at the time.
This was a very controversial statement at the time since the FDA pushed the drug on African migrants back in 2015, and the drug was praised in several scientific journals.
A group of brave doctors had filed a federal lawsuit against the U.S. Department of Health and Human Services (HHS) and the Food and Drug Administration (FDA) over the agencies’ unlawful attempts to block the use of ivermectin in treating COVID-19.
The lawsuit, filed in the U.S. Southern District of Texas in Galveston, argues that the FDA has overstepped its authority and unjustifiably interfered with their medical practice.
The plaintiffs, Drs. Mary Talley Bowden, Paul E. Marik, and Robert L. Apter, are contesting the FDA’s portrayal of ivermectin as dangerous for human consumption. They note that the FDA has approved ivermectin for human use since 1996 for a variety of diseases. However, they allege that with the advent of the COVID-19 pandemic, the FDA began releasing documents and social media posts discouraging the use of the anti-viral drug for COVID-19 treatment.
“We’re suing the FDA for lying to the public about ivermectin,” said Dr. Bowden.
They couldn’t make any money on it so they outlawed it and talked trash about it. A few of us found it anyway and took it. We were right all along. Some of them should be charged with murder as it would have saved lives
A team of Japanese researchers analyzed blood transfusions taken from individuals who were previously inoculated with COVID-19 vaccines. The researchers found that experimental COVID-19 vaccines destroy the continuity and biochemistry of human blood in six key areas. The vaccine damage is so significant; the contaminated blood can further damage unvaccinated and vaccinated people who receive blood transfusions or organ transplants from the vaccinated. The researchers published a pre-print paper on their findings and make suggestions for specific tests, testing methods and regulations to help deal with these risks.
Now the researchers are sounding the alarm about serious risks associated with using blood from people inoculated with COVID-19 vaccines. They are calling on the global medical community to put an end to these products.
“The health injuries caused by genetic vaccination are already extremely serious, and it is high time that countries and relevant organizations take concrete steps together to identify the risks and to control and resolve them,” the researchers wrote.
Six areas of blood contamination caused by COVID-19 vaccines
There are six key areas of blood contamination from vaccinated blood that researchers are concerned about:
Bombshell official government data has finally confirmed what many have long suspected – that Covid mRNA shots are responsible for skyrocketing cases of deadly cancers.
In the United States, cancer is the second leading cause of death.
The leading cause of death is heart disease, which has also spiked dramatically since Covid injections were rolled out for public use in 2021.
Now, new data shows that cancer has been on the rise as a result of the experimental Covid mRNA injections.
Official U.S. government data confirms the risk of developing cancer increases by a shocking 143,233% following Covid vaccination.
I am no longer a professor of medicine at Harvard. The Harvard motto is Veritas, Latin for truth. But, as I discovered, truth can get you fired. This is my story—a story of a Harvard biostatistician and infectious-disease epidemiologist, clinging to the truth as the world lost its way during the Covid pandemic.
On March 10, 2020, before any government prompting, Harvard declared that it would “suspend in-person classes and shift to online learning.” Across the country, universities, schools, and state governments followed Harvard’s lead.
Yet it was clear, from early 2020, that the virus would eventually spread across the globe, and that it would be futile to try to suppress it with lockdowns. It was also clear that lockdowns would inflict enormous collateral damage, not only on education but also on public health, including treatment for cancer, cardiovascular disease, and mental health. We will be dealing with the harm done for decades. Our children, the elderly, the middle class, the working class, and the poor around the world—all will suffer.
Schools closed in many other countries, too, but under heavy international criticism, Sweden kept its schools and daycares open for its 1.8 million children, ages one to 15. Why? While anyone can get infected, we have known since early 2020 that more than a thousandfold difference in Covid mortality risk holds between the young and the old. Children faced minuscule risk from Covid, and interrupting their education would disadvantage them for life, especially those whose families could not afford private schools, pod schools, or tutors, or to homeschool.
What were the results during the spring of 2020? With schools open, Sweden had zero Covid deaths in the one-to-15 age group, while teachers had the same mortality as the average of other professions. Based on those facts, summarized in a July 7, 2020, report by the Swedish Public Health Agency, all U.S. schools should have quickly reopened.
Of course it worked. That’s why they banned it. They couldn’t make a dime off a Nobel winning product that had gone past it’s patent expiration. The global power hungry people also couldn’t corral the sheep without the jab so they banned Ivermectin (and Hydroxycholoroquine).
Here’s the story
A new study discovered that people who tested positive for COVID-19 and took ivermectin as a treatment recovered faster than a comparison group.
According to a large study from the United Kingdom, the results of which were published by the Journal of Infection on Feb. 29, 2024, the time to self-reported recovery was a median of two days faster among the ivermectin recipients.
It was also revealed that the quicker recovery period was statistically significant.
In addition to that, people who received ivermectin were also less likely to be hospitalized or die. The study pointed out that 1.6% of ivermectin recipients were hospitalized or died versus 4% of the comparison group, which received typical care, which in the U.K. is largely focused on managing symptoms.
The study also found that ivermectin recipients enjoyed a reduction of severe symptoms and sustained recovery.
An open-label trial was covered by the study that involved 2,157 ivermectin recipients and 3,256 who received typical care from June 23, 2021, to July 1, 2022, with participants being randomized and reporting symptoms and recovery.
“The best revenge is massive success,” a quote often attributed to the iconic singer Frank Sinatra.
For Shelley Luther, who risked it all to keep her business operating during the COVID-19 lockdowns, achieving success by reforming the very bureaucratic system that almost broke her could represent the greatest vindication after her many trials.
Luther defeated incumbent State Rep. Reggie Smith, earning 53.42 percent of the vote in Tuesday’s primary election, according to KRQX.
I, for one, advocate we bring the carrot *and* the stick. Incentivize getting the vaccine however we like – ice cream, lotteries, literally whatever, I don’t care – and require vaccination to do, uh, non-essential things. Wanna go to a bar to watch the game? Passport. https://t.co/0vav22CaPk
Protect, my foot. Take the jab or resign, anything else is moral and ethical cowardice. You take an oath to protect citizens? You get vaxxed. Shameful that we have to say this. @TPSOperationshttps://t.co/i9HsOXqAyo
Per WSJ: “It’s official: CDC now says Covid is the flu.”
Can it be that we shut the world down creating incalculable damage to our economy and kids, and trampled on individual rights over a flu? Or is it that a small band of people went to extremes to cover up their Frankenstein…
It was always just a cold or flu. They used it as a political weapon to control both the masses and the election. The jab was a weapon against the populations. The CDC is lying
The Dark BLACK, Dark RED Heart (Third from Left, or 2nd from Right) WORKING 100% HARDER THAN IT SHOULD … 5 Mos post C-19 RNA/DNA GENETIC JABB.
"If your heart is having to work 46% harder than a non-vaccinated person's heart, for six months, that's 18 million beats… Every one of those beats is at close to 50% more energy required than a [unvaccinated] person's heart. It only happens after the vaccine."
Recent revelations from a source with knowledge of the matter suggest that the regime has mandated the nationwide destruction of all COVID-19 data within the healthcare system.
Recently, Mr. Chen (pseudonym) from Changsha, Hunan, disclosed to the Chinese language edition of The Epoch Times that his friend holds a leadership role in a local hospital. “He told me directly: the government is instructing health departments across the country to eradicate all COVID-19-related data, including information on the entire epidemic prevention process and vaccination records. They must obliterate all data without leaving a trace, and computer records must be deleted entirely,” said Mr. Chen.
Mr. Chen said the person said that the directive is nationwide.
Mr. Chen elaborated that the CCP’s demand entails “No data can be spared, neither on paper nor on computers. Records of vaccine administration are to be expunged, as well as records of nucleic acid testing and any embarrassing incidents that occurred during the entire epidemic prevention process.”
According to Mr. Chen, the authorities seek to erase this period from history, intending to prevent future generations from learning about these events as it signifies a government failure. He drew parallels to previous CCP leader Mao Zedong’s actions that resulted in the deaths of many Chinese people, actions that were intentionally omitted from historical records.
There is more at this link, but it kind of tells us the obvious. It was created with gain of function, the jab was a lie and didn’t stop anything, there was a coverup of what really happened and they don’t want the rest of the world knowing the truth and revolting against those who perpetrated this on us.
The CDC report has revealed that almost 500,000 Americans aged between 0 and 44 years old died from the dangerous side effects of the Covid mRNA injections between the start of the public rollout of the shots in early 2021 and October 9, 2022.
However, the shocking revelations from the report have been completely ignored by the corporate media – the same outlets that told the public the vaccines were “safe and effective.”
Compared to other countries, the U.S. Government has been slow to publish relevant and up-to-date data to allow the public to analyze the consequences of rolling out the Covid injections.
Of course it does. None of this is a surprise. The only real surprise is that people behind the jab aren’t in jail yet or are being charged with murder, but here goes.
Vaccines that protect against severe illness, death and lingering long Covid symptoms from a coronavirus infection were linked to small increases in neurological, blood, and heart-related conditions in the largest global vaccine safety study to date.
The rare events — identified early in the pandemic — included a higher risk of heart-related inflammation from mRNA shots made by Pfizer Inc., BioNTech SE, and Moderna Inc., and an increased risk of a type of blood clot in the brain after immunization with viral-vector vaccines such as the one developed by the University of Oxford and made by AstraZeneca Plc.
The viral-vector jabs were also tied to an increased risk of Guillain-Barre syndrome, a neurological disorder in which the immune system mistakenly attacks the peripheral nervous system.
More than 13.5 billion doses of Covid vaccines have been administered globally over the past three years, saving over 1 million lives in Europe alone. Still, a small proportion of people immunized were injured by the shots, stoking debate about their benefits versus harms.
The new research, by the Global Vaccine Data Network, was published in the journal Vaccine last week, with the data made available via interactive dashboards to show methodology and specific findings.
The research looked for 13 medical conditions that the group considered “adverse events of special interest” among 99 million vaccinated individuals in eight countries, aiming to identify higher-than-expected cases after a Covid shot. The use of aggregated data increased the possibility of identifying rare safety signals that might have been missed when looking only at smaller populations.
The more things change… and I don’t mean the Chiefs winning again.
Yay! Who doesn’t like setting records?
So we come to Sunday night.
Super Bowl 58 had been a snooze – fumbles, punts, more fumbles, it reminded me of nothing so much as a Jets game – but it was just getting good.
Then it went to commercial: a library… a portrait of Isaac Newton… an anatomy textbook…
Huh, I thought. This is weird –
Hey, wait, isn’t that a portrait of Karl Christian Friedrich “Charles” Pfizer – 19th century German-born chemist, founder of the company that bears his name?
Super Bowl spots this year cost a cool $7 million for 30 seconds (arguably a bargain, given that the biggest audience since the moon landing watched Sunday’s game). This ad ran a full minute, so $14 million. Plus production and licensing costs.
And, again, the ad doesn’t mention any specific products, except penicillin, which is not exactly a big Pfizer product these days. The reference to Katalin Kariko flicks at the Covid jabs. But I would guess only 5 to 10 percent of Americans have any idea who she is. Including her is a way to mention the mRNAs without talking about them.
Viewers know about turbo cancer, auto-immunity, the suppression of Ivermectin as the cure to Covid-19 and the damage the jab and mRNA causes. Those in the know hammered Pfizer for a public image commercial. Go read and understand that they aren’t fooling anyone except those wanting to be fooled.
Video GrammaFeb 13Could not agree more! I’m convinced that was a major factor to go all out to suppress ivermectin use. Sure getting the EUA was important, but short lived, compared to decades of cancer “treatments”. If there was wide spread ivermectin use, cancer rates & deaths would very noticeably reduce. Can’t have that! Isn’t the oncology racket about a $200 billion annual market now? 😔🤬
Alanna WilgusFeb 13Current cancer treatments are extremely toxic and marginally effective. The worst part is that the protocols bankrupt the patient and family. Meanwhile, they discredit cheap and effective treatments. Pharma and mainstream medicine are pure evil.
AKGFeb 13“Why blow $14 million-plus on what is essentially a generic corporate image campaign?” Because they can. Because our government gave them billions.
Harvard requires all students who will be on campus to have some protection from COVID-19 through vaccination. This may be through the initial primary series of COVID-19 vaccination or one of the most recent COVID-19 boosters. Vaccines must be FDA- or WHO-approved vaccines. As we work to continue the high levels of vaccination needed to protect our community, Harvard highly recommends being up-to-date per the CDC definition for all Harvard community members, including faculty, students, staff, and researchers, who will have any on-campus presence.
Wow, the whole world knows now that the only thing the jab is good for is controlling the sheep who comply. Who would want to hire someone like that out of college?
Researchers have published the results from a troubling new study that confirms Covid mRNA shots are responsible for spikes in serious and potentially fatal health issues.
The groundbreaking study found direct links between the injections and cases of vaccine-acquired immunodeficiency syndrome (VAIDS), various types of cancer, heart failure, and brain disorders.
The study’s paper was reported by Thailand’s leading English-language corporate media outlet, the Bangkok Post.
The researchers found that people who receive multiple Covid injections, i.e., a double dose of mRNA shots from Pfizer-BioNTech followed by a “booster,” can cause all sorts of health horrors to manifest, potentially resulting in sudden and early death.
(The Epoch Times)—With considerably lower efficacy rates, mRNA COVID-19 vaccines cause more deaths than save lives, according to a new study whose researchers called for a “global moratorium” on the shots and “immediate removal” from childhood immunization schedule.
The peer-reviewed study, published in the Cureus journal on Jan. 24, analyzed reports from the initial phase 3 trials of Pfizer and Moderna COVID-19 mRNA vaccines. These trials led to the shots being approved under Emergency Use Authorization (EUA) in the United States. The study also looked into several other research and reviews of the trials. It found that the vaccines had “dramatically lower” efficacy rates than the vaccine companies claimed.
Moreover, based on “conservative assumptions, the estimated harms of the COVID-19 mRNA vaccines greatly outweigh the rewards: for every life saved, there were nearly 14 times more deaths caused by the modified mRNA injections.”
It only took four years, the courage of a handful of independent medical experts who risked their careers by contradicting the federal government, the mainstream media, and the medical establishment, and the fact that something resembling the free press remains viable in this country, thanks largely to the internet.
Now, finally, the truth about the COVID-19 vaccine is beginning to be made known to the public. It confirms the many previous warnings such as these: here, here, and here.
It’s a research paper entitled “COVID-19 mRNA Vaccines: Lessons Learned from the Registrational Trials and Global Vaccination Campaign” that appeared on the internet at the Cureus Journal of Medical Science. The abstract bears your close reading and then re-reading, especially if you are one of the millions of Americans who did what public health gurus like Dr. Anthony Fauci incessantly told us to do and “followed the science.”
Here’s the abstract, but I’ve broken it into multiple paragraphs to aid your reading, and I’ve included my own emphasis of highlights (it is one long paragraph on the website):
Our understanding of COVID-19 vaccinations and their impact on health and mortality has evolved substantially since the first vaccine rollouts. Published reports from the original randomized phase 3 trials concluded that the COVID-19 mRNA vaccines could greatly reduce COVID-19 symptoms. In the interim, problems with the methods, execution, and reporting of these pivotal trials have emerged.
Re-analysis of the Pfizer trial data identified statistically significant increases in serious adverse events (SAEs) in the vaccine group. Numerous SAEs were identified following the Emergency Use Authorization (EUA), including death, cancer, cardiac events, and various autoimmune, hematological, reproductive, and neurological disorders. Furthermore, these products never underwent adequate safety and toxicological testing in accordance with previously established scientific standards.
Among the other major topics addressed in this narrative review are the published analyses of serious harms to humans, quality control issues and process-related impurities, mechanisms underlying adverse events (AEs), the immunologic basis for vaccine inefficacy, and concerning mortality trends based on the registrational trial data.
The risk-benefit imbalance substantiated by the evidence to date contraindicates further booster injections and suggests that, at a minimum, the mRNA injections should be removed from the childhood immunization program until proper safety and toxicological studies are conducted.
What those of us who opened their eyes know. It was a lie to begin with, it didn’t stop transmission or prevent Covid, It kills people and those behind it committed crimes against humanity.
And finally to Mr. Pfizer Travis Kelce, I hope the money was worth it. You already have to put up with Taylor, the celebrity bicycle that many have ridden. Now, you have to live with the uncertainty of health issues. Enjoy
“For the first time in a published and peer-reviewed paper, scientists are calling for a ‘global moratorium on modified mRNA products’ after surveying data from Pfizer’s and Moderna’s COVID-19 ‘vaccine” trials.'”
“The scientists found that the trials were rushed, presented low efficacy, were contaminated with residual DNA impurities, and that the ‘vaccines’ present many ‘biological mechanisms’ that can cause serious adverse events. The authors also advised the COVID shots should be removed from the Childhood Adolescent Immunization Schedule until proper safety studies are conducted,” the report confirmed.
Stunningly, the study provided a “generous estimate” that two lives were saved from COVID for every 100,000 shots.
The sports journalism community is mourning the sudden passing of Mike Dickson, a prominent figure in tennis reporting. Dickson, who was set to celebrate his 60th birthday on January 27, died suddenly while in Melbourne for the Australian Open.
The news of his death was confirmed through a social media post by his wife and children. “We are devastated to announce that our wonderful husband and Dad, Mike, has collapsed and died while in Melbourne for the Aus Open,” read the message shared via Dickson’s X account. “For 38 years, he lived his dream covering sport all over the world. He was a truly great man, and we will miss him terribly,” added the message from “Lucy, Sam, Ruby, and Joe.”
While generally respected in the sports journalism space, Dickson was also the author of many stories shaming and trying to cancel tennis star Novak Djokovic.
With all the died suddenly stories and vaxxed people keeling over, you’d think someone would have the guts to say we were wrong about the jab. They can’t say the truth that would go like this, it was a de-population tactic on the scale never tried before with an untested jab based on monetary gain rather than medicine or science.
Novak is a hero for standing up for the truth, and seeing through the bullshit that the media, the pharma companies and the world governments tried to tell us.
For those who are not doctors, which happens to be most of us, we depend on those few who have dedicated years of their lives to the scientific and medical fields to help inform us so we can make good decisions about our own health. Heading into the pandemic, a public largely jaded toward media and the government still placed high trust in their doctors. That trust has largely been betrayed during the Covid-19 pandemic years. CDC and FDA consultant Dr. Paul Offit’s response to concerns that the mRNA Covid shots may not be safe is an example of that betrayal.
In this specific case, the Florida Surgeon General, Dr. Joseph Ladapo, called for an end to the use of Pfizer and Moderna mRNA Covid-19 shots, due to the discovery of DNA fragments in the vaccines, including the SV-40 promoter, which is associated with cancer. The concern is integration, which is when foreign DNA becomes incorporated into chromosomal DNA, becoming part of the human genome.
Dr. Ladapo wrote to the FDA on December 6, 2023 asking if the proper assessments have been conducted on the mRNA shots to address the following risks, identified by the FDA in a 2007 publication about plasmid DNA vaccines:
DNA integration could theoretically impact a human’s oncogenes – the genes which can transform a healthy cell into a cancerous cell.
DNA integration may result in chromosomal instability.
The Guidance for Industry discusses biodistribution of DNA vaccines and how such integration could affect unintended parts of the body including blood, heart, brain, liver, kidney, bone marrow, ovaries/testes, lung, draining lymph nodes, spleen, the site of administration and subcutis at injection site.
Support of Black Lives Matter and calls to defund the police reverberated across America in 2020 following the death of George Floyd, igniting social justice protests and riots at a time when the coronavirus and lockdowns upended society in unprecedented ways. What was left in 2020’s wake was a massive increase in the number of murders, dealing a disproportionate blow to Black Americans.
“Certainly, the protests and riots mid-2020 after the death of George Floyd followed a pattern of spiking violence that we’ve seen following past viral police incidents, such as the deaths of Michael Brown and Freddie Gray. This pattern has been termed the ‘Ferguson Effect’: police pull back while violent crime spikes precipitously,” Hannah Meyers, director of the policing and public safety initiative at the Manhattan Institute, told Fox News Digital.
I’ve got news for you, the riots had nothing to do with Covid and had a lot to do with looting and destroying. More breaking news, 90% of this crime is black on black and less than 2% is cop shootings.
It’s because the people committing the crimes want to do it. They are shooting those they want to shoot, not because of a skin color (this is black on black we are talking about, although there is a significant black on Asian crime trend occurring). They are looting because they don’t want to work to pay for a TV.
Of course blaming the cops and whites on this is convenient for the race hustlers like Joy Reid, Whoopi Goldberg, Trevor Noah, Al Sharpton, both Obama’s, Eric Holder, all major news sources in any media format and the whole Biden Administration and those looking to get elected in November and have a D next to their name.
I don’t know how much longer the lies can be either hidden or perpetuated by Twitter, Fake book, screw tube, Google and other censorship leaders in the Tech industry.
Also not discussed is the problem that Obama called out in 2008, the lack of Fathers in black families. Men need other men to be taught how to act, especially when it is tough growing up and you are trying to figure out life. If your only role model is a street thug, guess what your life is headed towards?
What is real racism?
Let’s not forget that there is some real racism all over the place, like those who kill others based on skin color. No, it want a lynching or a fake NASCAR garage pull for Bubba Wallace Smollet. That got 15 FBI agents and how many are in New York right now? The big goose egg, except for those covering up the real story in the press
As Team Biden searches furiously for those touched by this supposedly ubiquitous white threat, black racists scream hatred and inflict dozens of casualties, some fatal.
The NYPD says that Wednesday, a black man named Frank James unleashed a smoke bomb on a Brooklyn subway train. He then fired 33 rounds from a Glock pistol. James allegedly shot 10 commuters, and 13 suffered other injuries. Five were hospitalized in critical condition. Amazingly, no one was killed.
Why did James do this?
Journalist Andy Ngo perused his social-media profile. James’ profane, deeply bigoted posts foreshadow an atrocious, anti-white hate crime.
He posted this, which is not being reported:
* “O black Jesus, please kill all the whiteys,” James wrote on Facebook.
* “The white motherf–kers that I want to kill, you know, I really want to kill them because they’re white,” James declared.
* “White people and black people as we call ourselves should not have any contact with each other,” James stated. “Blacks and whites so-called should not even be in the same hemisphere.”
Frank James had nine prior arrests in Gotham and three in New Jersey.
Meanwhile, police in Waukesha, Wis., report that Darrell Edward Brooks in November plowed his Ford Escape SUV into marchers and spectators at a Christmas parade. Brooks’ carnage killed six people and wounded 62 others.
Brooks also is an outspoken, white-hating bigot. All of this on Fascist book who hasn’t suspended him, but yet finds time to hate anyone they want who is not liberal.
If you can find the source, I’ll credit it. It was lost in translation
Since April 2022, the unvaccinated fared better than the COVID vaccinated from a mortality perspective (this could be true earlier than April 2022, but I currently lack the data to show this): there were no COVID “humps” and the seasonal increase in mortality was lower than for the vaccinated.
COVID hasn’t been killing anyone since April 2022 in any significant numbers. This means that there was absolutely no reason for anyone to get a booster shot after April 2022. Even if the vaccine were safe and worked perfectly, there is no data supporting such a need.
The flu vaccines have a “Day 0” mortality rate that exceeds the “1 excess death per M doses” criteria for a safe vaccine. The flu vaccines are clearly unsafe and should be immediately pulled from the market. Flu vaccines also have no hospitalization benefit whatsoever as was pointed out in a JAMA paper published in April 2023. The flu shots simply kill people for no benefit. The data is in plain sight for all to see.
The CDC never cites the Medicare data as proof of vaccine safety and efficacy for any vaccine because the data shows the opposite. All data is kept hidden from public view. So you’ll never see any of the graphs shown in this article from the CDC even though they have the data. They basically only publish data that fits the narrative.
The mRNA COVID vaccines should be pulled from the market. They are literally doing the opposite of what was promised.
The flu vaccine should be pulled as well. While the flu vaccine isn’t nearly as deadly as the COVID vaccine, it is an unsafe vaccine with no measurable clinical benefit.
The man who sold his soul for fame admitted another Covid lie. It seems that most of the restrictions was about controlling the masses, disrupting elections and personal wealth for some.
Fauci, 83, revealed to the House Select Subcommittee on the Coronavirus Pandemic that the “six feet apart” recommendation championed by him and other US public health officials was “likely not based on scientific data,” according to Chairman Brad Wenstrup (R-Ohio), who is also a physician.
Schools nationwide remained closed well into the second year of the pandemic as a result of the social distancing guidelines, which were disputed by both research studies and other health officials.
“It never struck me that six feet was particularly sensical in the context of mitigation,” Dr. Ashish Jha, the dean of the Brown University School of Public Health who served as President Biden’s COVID response coordinator for 15 months, told the New York Times in March 2021.
A world-renowned biologist has blown the whistle with explosive allegations against globalist power elites and the pharmaceutical industry.
Biologist Bret Weinstein dropped several bombshells during a new interview with independent news anchor Tucker Carlson.
While raising the alarm about the power grab of the United Nations (UN) World Health Organization (WHO), Weinstein left Carlson stunned when he stated how many people have died from Covid mRNA injections.
He cited scientific evidence that shows 17 million died globally as a result of the shots.
“So I’m not a math genius, but one in eight hundred shots times billions is a lot of people…17 million deaths from the Covid vaccine?” Carlson asked.
“Just for perspective: I mean, that’s like the death toll of a global war,” Carlson noted.
You begin to wonder whether the government is really out to get us or is just dumb as shit. The conspiracist in me remembers Covid and the 2020 elections. Lock everyone down while committing crimes, the old magicians watch my hand and not the door behind me trick.
Well, they’ve got a new list of stuff to scare the under educated with. The reason I question it is that the hotbed is the United States when in fact a lot of the shady practices are known to be in China.
Between 2000 and 2021 at least 16 pathogens reportedly escaped from research laboratories, according to a new study published in The Lancet Microbe — but the study authors said their findings may “only represent the tip of the iceberg” in terms of numbers due to a lack of standard reporting requirements.
A team of researchers surveyed peer-reviewed articles and online reports in English, Chinese and German, looking for all indications that a pathogen accidentally “escaped” from a lab or that an infection was determined to be “laboratory-acquired” during the study period.
In addition to the 16 episodes of pathogenic “escape,” the researchers found 309 instances of lab-acquired infections caused by 51 different pathogens.
Seventy-seven percent of those infections were caused by bacterial pathogens, 13.9% were caused by viruses, 7.1% by parasites, 1.6% by fungi and less than 1% by a prion agent.
Eight of the cases were fatal, and six of those deaths were caused by bacteria, such as Yersinia pestis, which causes plague, or Neisseria meningitidis. One death was caused by Ebola virus.
The vast majority of infections occurred as an outcome of “procedural errors,” breaches of biosafety or risk mitigation procedures, which included using the wrong personal protective equipment, having inadequate training or mishandling samples.
Needlestick injuries, spills, splashes, open vials, animal bites or “unknown reasons” caused the remainder of the infections.
Most illnesses occurred in North America, Europe and Asia with the U.S. accounting for more than three-quarters of the infections. The majority of pathogen escapes were “internal,” meaning they were confined to the lab, but a few escaped into the broader community.
I’m not surprised that the CDC and the NIH are behind a lot of this. They were behind us having to bend over and taking it in the ass over Covid. They are taking away freedoms from us one at a time, like being pecked to death by a pack of ducks
The bullshit that is spewed from Washington, the current White House, the MSM, anyone connected to Covid and the upcoming elections, so we need to know how to figure out the truth. If you don’t want to read, the answer is usually the opposite of whatever they are trying.
If they are accusing someone of something, it is what they are doing.
The current status quo on racism for example is that only white, conservative, Christian, republican men are racist and/or can be discriminated against.
For the entire time since the Civil war, it has been the democrats, the MSM and the woke who mostly are responsible for racism and discrimination. We had almost put racial identity politics behind us until Obama and Holder divided the nation.
It makes us cringe when we hear black Americans praise Lyndon B. Johnson and talk about how he passed the Civil Rights Act and signed it into law. He was a known racist. The crazy thing is, some sources also attribute this quote to Johnson: “We will have those n-word’s voting Democrat for the next 200 years.” So while he was signing the Civil Rights Act into law with one hand, he was unapologetically spewing racist words and trying to control the black vote with the other hand.
He didn’t care about blacks.
Now, anything that is not from the left or if they don’t get their way is racist.
Joy Reid, Shiela Jackson Lee, Kamala Harris, Maxine Waters, Lewis Hamilton, Bubba Wallace, Colin Kaepernick, Don Lemon, MSNBC, CNN, Whoopi Goldberg, Lebron James, Jussie Smollet and the Squad have all cried racism, when in fact they have been the racist ones.
Joe Biden has a list a mile long of racist remarks, yet uses it when he doesn’t get his way, like the recent speech on the voting bill. He quoted Jefferson Davis, George Wallace as what we were if we didn’t support him. Davis was a democrat. Biden was friends with Robert Byrd, Grand Cleagle of the KKK.
On 2/3/2022 Biden made this racist comment:
President Joe Biden referred to blacks as “colored” during a speech at the National Prayer Breakfast on Thursday during Black History Month.
Biden was telling the story of seeing “colored kids” on a bus when he moved from Scranton, Pa., to Claymont, Dela.
In context: Joe Biden, George Wallace, Bull Connor and Jefferson Davis are all Democrats.
both democrats and life long compatriots
Byrd in full uniform
Never forget what Democrats, & notably @JoeBiden, did to Janice Rogers Brown, Priscilla Owen – but more… Miguel Estrada. Destroying a good man specifically because he is Hispanic. We know this to be factually true, but the beltway media elites brush it aside. #RacistDCDemocratshttps://t.co/2KKXUUsWlr
The South in the Civil War were democrats. Slave owners were mostly democrats.
I can go on with this, but the pattern is there. It is those who cry racism because is is a cheap threat to get their way. They then make false claims that if said by a white male would be called racist, therefore what they say is racist. It’s logic.
2. It’s not a socialist agenda. The hell it’s not. The current Congress is trying to fix elections so they can stay in power, are making millions on insider stock trades (both parties) and pass laws to keep one class in power to rule the others. They want to take away guns, the start of a communist movement and regulate everything. (that is why they hated Trump so much, he took away their overbearing regulatory powers)
It says right on the BLM website that they are a Marxist organization. Bernie Sanders is a communist.
3. Collusion with Russia and China. After a 3 year circus which cost the taxpayers 30+ million dollars. We found out that Trump didn’t do anything. On the other hand, Hunter Biden is on the board of Burisma and is being bought by the Russians and the Chinese. Hillary sold the rights to much of our uranium to the Russians.
His whoring and drugging is well documented, but the MSM isn’t covering a bit of it. The FBI should be all over this, but they are protecting their own.
So if they say someone else is colluding, it is who is saying it.
4. The vaccine is the only cure to Covid and that it will cure Covid.
If you go to the Danish studies, or look at the vaccine failure in Israel, you can pretty much know that the jab has nothing to do with preventing either getting or spreading Covid. It’s a cover for a power grab.
Ending Covid
They have a plan to end Covid and Donald Trump doesn’t. They campaigned on not to take a trump vax, and claimed they weren’t left with any vaccines or plans when Trump left. Biden had plenty of vaccine supply (when we thought it worked) and a Plan (Operation Warp Speed) to handle it. Fucking it up was the Biden/Harris job.
Harris said she wouldn’t trust a jab that Trump developed. Now we should get 3 shots because it is the B/H vaxx now. Talk about a flip/flop.
3. Global Warming. This is a socialist agenda that is just another scare dreamed up to scam money. The biggest bullshitter was Al Gore.
Right now, countries are shutting off fossil fuels with no back up. Solar and wind energy have failed to provide what is needed and they are closing down nuclear plants. Now, prices are skyrocketing for fuel and that is all that is working.
men and women are equal – sports will be men and co-ed
Military needs to be woke – china laughing at us. military needs to defend country. goal is to kill and protect, not dress up
We need absentee voter pickup boxes,
It’s already been determined, from research by Rodney Doyle at the Caesar Rodney Election Research Institute in Irving, Texas, that the $419.5 million Mark Zuckerberg of Meta gave the Center for Technology and Civil Life and the Center for Election Innovation and Research essentially bought the 2020 election for Joe Biden.
Now there’s evidence that was the strategy all along, that the goal of such election manipulation had been birthed years before and ultimately used by extremists.
The procedure was that Zuckerberg handed over the money and leftist activists distributed it before the election – not in a nonpartisan fashion as some have claimed – but specifically to extremists like themselves who used it for get-out-the-vote efforts specifically aimed at benefiting Biden.
A new analysis at The Federalist, by Doyle, confirms that the money was used “to manipulate the 2020 election in favor of President Joe Biden.”
January 6th was an attack on democracy
Feminists will go all Karen on the USA, white men and discrimination in America, but will ignore women’s rights around the world where the oppression really takes place.
There is a lot of good reading here, the best insults, the best stories of fooling around at work, the biggest racists, history, IQ and more to catch up on.
A beer short of a six pack A brick short of a load A couple of eggs shy of a dozen A couple of gallons short of a full tank A few ants short of a picnic A few beers short of a six-pack A few bricks short of a pile A few bricks short of a wall
It’s a long list, click on it for your friends, and enemies
….Facts are facts, no matter how much you try to deny them, or how much you blame others for what you did. Here they are. Democrats are the Jim Crow party, KKK and the party behind eugenics – the attack on blacks by abortion. They have been behind the slavery, racism, bias, and are everything they accuse others of being and doing.
There are a lot of inconvenient (for Democrats and liberals) truths in this. It names names, lists who they are and what they did, meme’s to steal for the upcoming election and blows out of the water anything other than who they really are, including Biden.
….I found what I thought was a private place and parked. I made my move quickly as I figured we were drunk and if I got any push back, I’d just go home. I wasn’t going to try that hard. Well, she was in on the plan and probably hadn’t gotten any since college so her shirt was unbuttoned in no time. I’d had a steady college girlfriend who had the same bra that unsnapped in the front. I had it undone faster than Fonzie from Happy Days, to which her surprised response was wow, you did that well. I said I’d done it before, so she knew she was going to have a ride that night. Let the rodeo begin.
…..As I suspected, ha is a single word equating to “I’ll let you go now” the on phone or best wishes. I also means I don’t want to text anymore and this lets you think something witty was said while giving you the finger. I got news for you, it wasn’t. I knew what you meant which is why I don’t want to continue and doubt whether you are mature.
While this wasn’t written in 2023, it still got a ton of clicks because people want to know what it’s like to be smart.
….Since I published this, the comments have been coming in and are now far better than the blog post. I encourage you to read about the lives and struggles of those who have high IQ. Their stories are quite revealing.-> It’s in the comments, hint, hint, hint.
People still care about Covid-19 as this was written in 2020
….According to Sasha Latypova, a Russian-American, former pharmaceutical industry research and development executive, and Katherine Watt, a para-legal researcher, and philosopher, it’s an inside job. Covid-19 is an act of bio-warfare perpetrated by the U.S. Department of Defense (DoD) on the U.S. and worldwide populations in two stages.
That means that 29% are either under educated or believe what they are told and act like sheep.
There is enough evidence out there to show that it’s not safe and effective and in fact does damage. It’s killed more people than Covid-19 did.
I have friends and neighbors who are 4 jabs deep now. I found out you can’t tell people anything because they are going to believe what they want. I don’t even tell them I’m not because they don’t want to hear it. Some think they are protecting themselves, others just gave up and got it. That’s how effective the propaganda was. It was 1930 in Germany level of disinformation.
Anyway, here is the story:
After initially promising that the Covid vaccine would prevent Covid, then promising it would at least prevent transmission, then promising it would prevent illness, public health experts have had to admit all three promises are untrue. The government and pharmaceutical industry continue to press even healthy people and children to get formulations of Covid vaccines, each of which carries potential risks both known and unknown.
The following is from Sharyl Attkisson:
Less than one-third of Americans, 29%, have gotten the new Covid-19 vaccine that was released this fall. In contrast, 47% of U.S. adults say they have gotten the annual flu shot this year.
Another 20% of U.S. adults indicate they plan to get the new Covid-19 shot, which could bring the level of current vaccination against Covid-19 to close to half of Americans, but that still falls below the combined 63% who have gotten or plan to get the flu shot.
These results are based on Gallup’s latest Covid-19 survey update, conducted Nov. 30-Dec. 7 with more than 6,000 adult members of Gallup’s probability-based panel.
Gallup had found that over seven in 10 U.S. adults had received the earlier versions of Covid-19 vaccines, which were first available to the public in late 2020 and early 2021.
The past two years, booster shots to those initial vaccines were made available. The new shot can be given to people regardless of whether they have been previously vaccinated against Covid-19.
Older Americans, those aged 65 and older, are getting the updated Covid-19 shots at higher rates than the general population — 46% have already done so.
However, seniors are still more likely to have gotten the annual flu shot, with 68% saying they had.
This year, public health officials have also recommended that older Americans get vaccinated against respiratory syncytial virus, or RSV.
To date, 22% of U.S. seniors have gotten an RSV vaccination.
In addition to age differences, vaccine intentions for both Covid-19 and flu differ by party identification, but more so for Covid-19.
Whereas nearly half of Democrats (48%) have gotten the updated Covid-19 shot, 20% of political independents and 10% of Republicans have.
Eighty-two percent of Republicans say they will not get the updated Covid-19 shot.
Sixty-one percent of Democrats, 38% of independents and 35% of Republicans have gotten the flu shot this year. Half of Republicans, 52%, say they will not do so. (Continued…)
However, people have noticed the booster shots do not work as advertised. And the fact there is no discernible seasonal pattern to infections is also not helping the case for an “annual preventative shot,” as the pharmaceutical companies had planned.
Per Pfizer’s interim 2-month, Phase-3 data that they submitted to the FDA on November 20, 2020, Pfizer was measuring the effectiveness of their mRNA injection from preventing COVID-19 symptoms confirmed by a positive PCR-test versus placebo (aka, not getting injected with mRNA-LNPs).
You can see from the chart below (pulled directly from Pfizer’s FDA submission) that 8 out of 17,411 participants (0.05%) in the Pfizer mRNA injected group came down with COVID-19 symptomsconfirmed by a positive PCR-test within 2 months or less after their second mRNA shot, versus 162 out of 17,511 (0.93%) in the placebo group.
This morning, Pfizer disappointed investors by saying it expects sales of its mRNA Covid jab to plunge again in 2024. Annual sales of Pfizer’s shot and anti-Covid drug Paxlovid will fall 35 percent next year – on the heels of an 80 percent collapse this year.
The announcement is an embarrassment for Pfizer executives, marking the third time in only three months they have had to rachet down expectations for Covid sales.
Investors expect public companies to be able to predict their sales at least six months to a year in advance. But collapsing mRNA demand keeps catching Pfizer off-guard.
Kelce’s “two things at once” spot encourages people to take both flu and Covid jabs at the same doctor’s visit – unsubtly linking the mRNAs with old-style inactivated virus flu shots, which have far fewer side effects.
But would-be recipients have not been fooled. While mRNA demand has collapsed, demand for flu shots remains solid (despite strong evidence of their uselessness).
Only two years ago, the mRNAs were among the world’s most desirable products, and hipsters proudly branded themselves “Team Pfizer” or “Team Moderna.”
A new paper in a top scientific journal shows they accidentally cause our cells to create vast numbers of random misshapen proteins; no one has any idea how serious the risks of those might be
How scary is a new paper showing mRNA Covid shots accidentally cause our bodies to make many different proteins and not just the Covid spike, as the shot’s promoters have claimed for three years?
Scary enough the paper’s authors began spinning their work as soon as they put it out. University of Cambridge professor Anne Willis, the study’s co-senior author, told reporters that mRNA “technology is amazing and it’s going to be revolutionary… but we’ve just made it a whole lot safer going forward.”
In all, almost 10 percent of the proteins that the mRNA Covid jabs make the body produce appear to be “wrong,” rather than the intended spike protein.
In the Cell paper, the authors show that neither Covid-19 itself nor the DNA-based Covid vaccine from AstraZeneca produce similar proteins. The effect is limited to the mRNAs.
The authors also reported they could find a biological response to the wrong proteins in mice and in humans. They warned that these proteins “could activate T cells that target host cells,” and that their other effects “could include increased production of new B cell antigens.”
T and B cells form the core of our immune system. In other words, the mRNA jabs may accidentally cause the body to attack its own tissues, as well as make antibodies that don’t work against the spike protein.
The leaked data, comprising 4 million out of 12 million vaccination records in New Zealand, revealed alarming statistics. Kirsch’s analysis concluded that for every 1,000 mRNA vaccine doses administered, one person died prematurely. This risk was particularly pronounced in the over-60s demographic. He stressed that the quality of this data is high and contains millions of records, allowing for clear identification of a significant death signal.
Kirsch criticized the lack of analysis by health authorities and accused them of ignoring safety data. He called out the silencing of whistleblowers and the reluctance of epidemiologists to engage with the data. His arguments are supported by prominent academics like Yale professor Harvey Risch and UK professor Norman Fenton, who affirm the vaccine’s lethal risks.
Kirsch also noted a dose-dependent risk in the vaccines, with each subsequent dose seemingly causing more harm, although the fourth dose appeared to have a flattened death curve. He emphasized that the harm seems cumulative and doesn’t return to baseline post-vaccination.
Would 92% of American adults have gotten a Covid shot had they known the “vaccines” only offered a 0.85% reduction in risk? Would young men have taken the jab if they had known it did not prevent transmission?
Americans came to understand that the media campaigns supporting the shots were fraudulent. The touted benefits – preventing infection and transmission – were lies. In response, fewer than one in five Americans elected to receive “boosters” despite multi-billion dollar propaganda campaigns.
Texas Attorney General Ken Paxton has now brought a suit to bring accountability for the fraud that resulted in record profits for the pharmaceutical industry. Last week, he filed a complaint alleging that Pfizer misrepresented Covid vaccine efficacy and “conspired to censor public discourse” in violation of Texas’s Deceptive Trade Practices Act (DTPA).
Paxton alleges that the $75 billion Pfizer has raked in through sales of Covid vaccines were the “direct and proximate result” of the company’s deceit.
The DTPA requires Paxton prove two questions to succeed in his case. First, he must establish that the company lied or failed to disclose known information concerning its Covid vaccine. Second, he must prove that the company’s fraud was designed to promote sales of the shots.
According to the CDC, the COVID-19 pandemic has claimed the lives of over 1.15 million Americans. However, after nearly four years of death and economic carnage, there’s been an underwhelming effort to get to the bottom of where it originated, so this may never happen again.
Independent presidential candidate Robert Kennedy Jr. attests that COVID-19 originated from a laboratory in Wuhan, China. And that a deliberate cover-up by powerful individuals who stood to benefit financially and professionally obscured the truth from the world.
In an October 2023 lecture, David E. Martin, Ph.D., detailed how we can know that SARS-CoV-2 is a manmade bioweapon that has been in the works for 58 years
The virus called “coronavirus” was first described in 1965. Two years later, the U.S. and U.K. launched an exchange program where healthy British military personnel were infected with coronavirus pathogens from the U.S. as part of the U.S. biological weapons program
In 1992, Ralph Baric at University of North Carolina, Chapel Hill, took a pathogen that used to infect the gut and lungs and altered it with a chimera to make it infect the heart, causing cardiomyopathy. This research was part of the efforts to produce an HIV vaccine
In November 2000, Pfizer patented its first spike protein vaccine. Between 2000 and 2019, vaccine trials using this technology proved it was lethal, yet in the summer of 2020, the clinical trials for the SARS-CoV-2 shots went straight into human trials
mRNA spike protein was publicly described as a bioweapon 18 years ago. In 2005, at a conference hosted by DARPA and The Mitre Corporation, the mRNA spike protein was hailed as a “biological warfare-enabling technology,” i.e., a biological warfare agent
(Mercola)—The video above features a lecture David E. Martin,1 Ph.D., gave in Dornach, Switzerland, in late October 2023. Martin is a national intelligence analyst and founder of IQ100 Index, which developed linguistic genomics, a platform capable of determining the intent of communications.
This technology has allowed Martin to scan and review millions of patents, resulting in a paper trail2,3 that conclusively proves SARS-CoV-2 is a man made bioweapon that has been in the works for 58 years.
Unambiguous Admission of a Premeditated Plandemic
As he is now in the habit of doing, Martin opens his lecture with a quote by Peter Daszak, president of EcoHealth Alliance. During a March 27, 2015, forum on Medical and Public Health Preparedness for Catastrophic Events, Daszak noted4 that unless an infectious disease crisis is at an emergency threshold, it tends to be ignored.
“To sustain the funding base beyond the crisis, we need to increase public understanding of the need for MCMs (medical countermeasures) such as a pan-influenza or pan-coronavirus vaccine,” Daszak said, adding:5
“A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of the process.”
Great, wearing a mask made us even more stupid. The social media Karen’s and Chad’s are struggling for a triple digit IQ as it is. The Covid particle is so small anyway that a mask preventing Covid is as effective as a chain link fence is stopping mosquitos.
It was about controlling the masses anyway
Excerpt:
Findings from the study showed a substantial decline in executive function, which refers to higher-level cognitive skills governing control and coordination. Alongside this, the study’s cohort showed a marked decline in working memory, which is crucial for short-term memory storage and various cognitive processes.
“Significant worsening of executive function and working memory was observed in the first year of the pandemic across the whole cohort, in people with mild cognitive impairment, and in people with a history of COVID-19,” the authors wrote.
The negative impact on cognitive function persisted into the second year, notably concerning executive function across the entire cohort and working memory within specific subgroups.
Cognitive Decline
Key factors for this cognitive decline were identified via regression analyses. Those factors included the fact that, amid lockdowns, people were exercising less and consuming more alcohol across the entire cohort. These factors also contributed to more people experiencing loneliness and depression.
The authors noted that concerns were expressed about the neuropsychological effects of the pandemic social restrictions, with particular respect to the context of potentially increased dementia risk in older adults.
In its own analytical documents, the Pfizer corporation classified its experimental mRNA treatment (in this case, under the trade name Comirnaty) as “very highly hazardous”. It did not announce this finding publicly, nor did it endeavor to make potential recipients of the treatment aware of the risk. Not to inform patients of the dangers was highly illegal, but it didn’t matter — Pfizer is too big to punish. No one involved in the process will ever be held accountable. No one will go to jail. And the major players will go to their graves as extremely wealthy people.
Many thanks to Hellequin GB for translating this article from the German blog TKP:
Pfizer classifies its own C19 modRNA product as “highly dangerous”
The modRNA products are moved through the body with the help of so-called lipid nanoparticles and transfected into the cells. The two lipids used by Pfizer, ALC-0159 and ALC-0315, had no approval before 2020 except for “research purposes”. In Pfizer’s safety data sheets they are assigned a medium toxic potential; in the syringe they cause a “high toxic potential.” It’s unbelievable that the authorities would allow something like this to be injected into the upper arms.
TKP published a detailed analysis on December 9, 2021. It quotes the company that produces these lipids. She writes on her website: “ALC-0159 is one of the components of the BNT162b2 vaccine against SARS-CoV-2, along with ALC-0315, DSPC and cholesterol. This product is for research use only and not for human use.”
And further: ALC-0159 and ALC-0315 are discussed in the EMA Assessment Report for the first conditional marketing authorization starting on page 22.
It says:
“All excipients except the functional lipids ALC-0315 and ALC-0159 and the structural lipid DSPC comply with the Ph. Eur. The functional lipids ALC-0315 and ALC-0159 are classified as novel excipients. The two structural lipids DSPC and cholesterol are used in several finished products that have already been approved.”
Here is the whole Thing. But not getting the jab in the first place was the better decision.
Excerpt below.
Congressional Research Service SUMMARY Compensation for COVID-19 Vaccine Injuries More than 260 million Americans, and billions of people worldwide, have received one or more doses of a vaccine to protect against Coronavirus Disease 2019 (COVID-19). Most common side effects of COVID-19 vaccines are mild and generally resolve in a few days. In rare instances,COVID-19 vaccines can cause serious adverse events.
Individuals who believe they are injured by COVID-19 vaccines may seek compensation for those injuries and associated harms or costs. Absent an applicable federal law, individuals allegedly injured by a vaccine might seek redress by filing a state tort law claim against the vaccine manufacturer. However, federal law has two distinct compensation regimes that limit legal liability for vaccine manufacturers and provide potential compensation—without requiring a showing of fault—for individuals harmed by adverse reactions to vaccines.
For injuries and deaths associated with most vaccines recommended by the Centers for Disease Control and Prevention (CDC) for routine administration in the United States , the National Vaccine Injury Compensation Program (VICP) may provide compensation. During public health emergencies declared under the Public Readiness and Emergency Preparedness Act (PREP Act), the Countermeasures Injury Compensation Program (CICP) may provide compensation for injuries and deaths resulting from the administration of “covered countermeasures,” which may include vaccines.
The VICP and CICP regimes are similar in some ways, but the programs serve distinct purposes. Compensation through CICP is generally less comprehensive than through VICP. CICP is a regulatory process administered by the Health Resources and Services Administration (HRSA), a division of the U.S. Department of Health and Human Services (HHS). CICP compensation is available only for death or serious injuries resulting from a covered countermeasure. A claimant must generally file a request form and associated documentation with HRSA within one year of the date that the covered countermeasure was administered. For injuries not listed by the Secretary of HHS on a Countermeasure Injury Table, the claimant must demonstrate that the injury was a direct result of the countermeasure’s administration based on compelling medical and scientific evidence. HRSA makes decisions regarding eligibility and compensation; judicial review is not available. CICP compensation is limited to reasonable medical expenses, loss of employment income, and a death benefit when the claimant’s death is a direct result of the administration of a covered countermeasure.
Under the Secretary of HHS’s current PREP Act Declaration for COVID-19, FDA-authorized or -approved COVID-19 vaccines are covered countermeasures. While a PREP Act declaration is in effect, CICP is the sole remedy available for injuries related to covered countermeasures, so CICP—and not VICP—will apply to injuries resulting from COVID-19 vaccinations while the Declaration remains in effect. Due to COVID-19, the number of CICP claims has increased dramatically. As of February 1, 2023, CICP has received 11,252 claims alleging injury or death relating to COVID-19 countermeasures. Of those, 8,067 claims (71.7%) relate to COVID-19 vaccines. HRSA has not yet compensated any CICP claims relating to COVID-19 countermeasures.
When coverage under the PREP Act Declaration for COVID-19 ends, COVID-19 vaccine injuries could be compensated through VICP, contingent on additional regulatory and statutory changes. To be included in the VICP, (1) the vaccine must be recommended by the CDC for routine administration to children or pregnant women; (2) the vaccine must be made subject by act of Congress to the excise tax that funds VICP; and (3) the Secretary of HHS must add the vaccine to the Vaccine Injury Table, which lists injuries and conditions associated with vaccines covered by VICP. Should all of these changes occur, COVID-19 vaccines would be covered by VICP.
To receive compensation through VICP for a vaccine-related injury or death, the injured person or their estate must file a petition with the U.S. Court of Federal Claims, generally within three years of the onset of the first symptom or significant aggravation of the injury, or within two years of death or four years of the first symptom resulting in death. To receive compensation, petitioners must show either that they experienced an injury listed in the Vaccine Injury Table within the time frame specified in the Table, or prove that the vaccine was the “but-for” cause of their injury. Special masters determine eligibility and compensation; their decisions may be appealed to the U.S. Court of Federal Claims and the U.S. Court of Appeals for the Federal Circuit. Successful petitioners may receive medical expenses, lost income, a set death benefit, and reasonable attorneys’ fees and costs. Petitioners who are dissatisfied with the compensation they receive, or whose claims are delayed, may opt to pursue civil actions in court, subject to certain limitations on vaccine manufacturer liability.
New research: COVID vaccinations led to millions dying
Exclusive: Chuck Norris offers dozens of links to data implicating Fauci, CDC, Pfizer, others
By Chuck Norris Published November 13, 2023 at 12:56pm
Over the past several months, I’ve been barraged with scientific studies and previously undisclosed government documents which have shown that COVID vaccinations led to millions of deaths, and continues to.
I was compelled to pass this research along to Americans and all the people of the world, whom I love dearly, to allow them to make up their own minds. Especially important is the video at the end of this column by an international banker who is dying from the COVID vaccines, along with his mother. Please watch it after you read the below evidence that gives the exact reasons he says what he does in the video.
Here’s just a small sample of recent studies and reports showing the detrimental effects of COVID vaccines around the country and world:
“A new scientific report challenges the idea that COVID-19 vaccines have prevented deaths after researchers assessed all-cause mortality in 17 countries and found that COVID-19 vaccines didn’t have any beneficial effect on reducing mortality. Instead, researchers found that unprecedented peaks in high all-cause mortality in each country – especially among the elderly population when COVID-19 vaccines were deployed – coincided with the rollout of third and fourth booster doses.”
“Conservative public interest advocacy group Defending the Republic (DTR) has obtained almost 15,000 pages of Moderna’s COVID-19 vaccine clinical trial data, claiming the data show an ‘utter lack of thoroughness’ of the trials and calls the vaccine’s safety into ‘serious doubt.'”
“A top Pentagon official has confirmed that cases of myocarditis soared among U.S. service members in 2021 after the COVID-19 vaccines were rolled out.”
“COVID-19 cases among vaccinated seniors soared in 2021, according to newly disclosed data acquired by U.S. health agencies but not presented to the public. Humetrix Cloud Services was contracted by the U.S. military to analyze vaccine data. The company performed a fresh analysis as authorities considered in 2021 whether COVID-19 vaccine boosters were necessary amid studies finding waning vaccine effectiveness. Humetrix researchers found that the proportion of total COVID-19 cases among the seniors was increasingly comprised of vaccinated people, according to the newly disclosed documents.”
According to an analysis, published this month in the International Journal of Vaccine Theory, Practice, and Research, of Pfizer-BioNTech COVID-19 vaccine clinical trial data, the vaccine makers hid fatality data from regulators in order to qualify for Emergency Use Authorization.
Pfizer-BioNTech delayed reporting vaccine-associated deaths among BNT162b2 clinical trial participants until after the U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) for the product.
The vaccine makers also failed to account for a large number of subjects who dropped out of the trial.
The authors of the paper described it as a “forensic analysis,” defined by the U.S. National Institute for Standards and Technology as “the use of scientific methods or expertise to investigate crimes or examine evidence that might be presented in a court of law.”
What the analysis shows
Corinne Michels, Ph.D., retired distinguished professor of biology at Queens College, New York, led the DailyClout Pfizer/BioNTech Documents Investigations Team on what the authors claim was the first independent examination of original data from the Pfizer-BioNTech COVID-19 mRNA vaccine (BNT162b2) clinical trial.
Investigators looked at each of the 38 deaths occurring between July 27, 2020, the start of phase 2/3 of the Pfizer-BioNTech vaccine trial, and March 13, 2021, the end date culminating in Pfizer-BioNTech’s 6-month interim report.
This trial phase involved 44,060 subjects. Half received a dose of BNT162b2, half got a placebo consisting of an inactive sterile salt solution.
The trial was unusual because at week 20 after the FDA issued the EUA for the vaccine, trial subjects in the placebo group were allowed to switch to the vaccinated group and receive their first BNT162b2 shot.
Switching from the placebo to the vaccinated group — or “unblinding” — normally occurs when the benefit of the drug is so great that not treating subjects becomes unethical. For example, investigators might consider unblinding a cancer trial if at some point all untreated patients deteriorated or died but all treated patients improved.
Unblinding conditions may be specified in the study design, but they usually involve input or review from medical ethicists.
Of 20,794 unblinded placebo subjects in the Pfizer trial, 19,685 received at least one dose of BNT162b2.
Normally the decision to unblind a vaccine trial would be based on the product’s safety and effectiveness in reaching certain endpoints or objectives. Endpoints for a drug to prevent viral infections might be a positive test or self-reported COVID-19 illness (the “case” numbers that drove much of COVID-19 policy), illness requiring hospitalization or death.
But, perhaps unexpectedly, after 33 weeks the data revealed no significant difference between deaths in the vaccinated and placebo groups for the initial 20-week placebo-controlled portion of the trial.
After week 20, after most former placebo subjects had received the vaccine, deaths among those in the vaccine group continued unabated.
The authors revealed “inconsistencies” between data presented in Pfizer-BioNTech’s 6-month interim report and subsequent publications by Pfizer-BioNTech trial site administrators:
“Most importantly, we found evidence of an over 3.7-fold increase in the number of deaths due to cardiac events in the BNT162b2 vaccinated individuals compared to those who received only the placebo.”
This means that 79% of relevant deaths were not recorded in time to be included in Pfizer’s regulatory paperwork.
By not including relevant subject deaths in the case report, Pfizer obscured cardiac adverse event signals, allowing the EUA to proceed unchallenged.
How did Pfizer get around legal, ethical obligations?
The Pfizer-BioNTech data, obtained through a Freedom of Information Act lawsuit, uncovered four additional deaths in the vaccine group and one more in the placebo group — but Pfizer failed to include these data in their FDA submission despite an explicit study design requirement to do so.
These data, and how they differ from what Pfizer-BioNTech reported in their applications, are summarized in Table 3 of Michels’ study.
One case involved a 63-year-old woman who died 41 days after receiving the shot, but whose death only entered the data pool 37 days later. Another was a 58-year-old woman whose death 72 days after vaccination went unreported for 26 days.
Had Pfizer-BioNTech met their legal and ethical obligation to report all serious adverse events their data would have shown equal deaths in placebo and vaccine groups — which would have shown no clear benefit for the vaccine.
How were they able to skirt those obligations?
For one, they were able to hide behind the the 2005 Public Readiness and Emergency Preparedness (PREP) Act, which provided an almost impenetrable liability shield for vaccine manufacturers for “medical countermeasures” in response to any “public health emergency.”
Second, because COVID-19 was viewed as a national health emergency, regulators abandoned the established, patient-centered, safety-based approval process requiring years of preclinical animal testing — and Pfizer-BioNTech unsurprisingly went along.
Timing of death reports raises questions
Michels also raised issues regarding total death reports and their timing.
Since the death total from both study groups, 38, appeared “surprisingly low” to study authors — particularly during a pandemic — they undertook their own analysis based on population mortality expectations at the time.
Assuming that age-adjusted death rates for the study subjects were similar to those of the general population, they estimated that 222 subjects should have died from July 27, 2020, to March 13, 2021. The reported number, 38, is just 18% of the expected number.
Michels explained this by the large number, 4.2% of “discontinued subjects.” The most concerning of these were subjects “lost to follow-up,” which means missing scheduled visits or other required activities.
Pfizer-BioNTech tried to reach these subjects via phone, certified mail or through their emergency contact but despite their efforts could not account for 395 subjects who had dropped out.
The authors wrote:
“These are not insignificant numbers and could easily account for the low number of deaths reported in this safety period of the trial. Given the importance of knowing the status of each trial subject, there should have been greater effort to locate these individuals.
“Additionally, Pfizer/BioNTech was responsible for oversight of the trial sites. Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Michels was also concerned over how certain trial centers had many dropped-out subjects while others had none or just a few.
Ninety-six of 153 trial sites (63%) reported 0 or 1 subjects lost to follow-up and 34 (22%) reported 2-5 dropouts. But four sites reported more than 20 subjects lost to follow-up, amounting to about 5% of all trial subjects.
Since the vaccine makers were responsible for trial site oversight, the authors wrote, “Sites with excessive numbers of lost to follow-up should have been evaluated for performance.”
Finally, based on the data, it appears Pfizer-BioNTech was in no hurry to enter death reports before the EUA submission deadline, particularly for the BNT162b2 group.
Of the 38 reported deaths only one case was added on the day the subject died. Delays of 20+ and 30+ days were common.
One death took 72 days to find its way into the database, and all were entered as occurring on the reporting day, not on the actual date of death.
Of the eight subjects in the vaccine group that should have been reported by Dec. 10, 2020, the EUA application cutoff, the average reporting delay was 17.5 days for subjects in the vaccine group, but just 5.9 days for deaths among subjects in the placebo group.
Look at the last sentence where other riders had to cut their career short. No mention of the obvious though.
Continental rider Mark Groeneveld has died of a suspected cardiac arrest, aged just 20, hours after competing in a race, his X-Speed United team has confirmed.
X-Speed United described Groeneveld as a “cherished member” of the team and someone with a “remarkable spirit” and an “infectious smile.” He had been with the team for the 2023 season, his first year racing at Continental level.
The Dutch rider had been in Hong Kong this week to compete at the Hong Kong Cyclothon, which was won by Jayco-AlUla’s Lukas Pöstlberger, but was forced to abandon the race as a result of a mechanical problem.
According to a report by the Dutch local newspaper, Noordhollands Dagblad, Groeneveld collapsed a while after the race and could not be resuscitated by paramedics. The team said it was working with authorities to determine the cause of Groeneveld’s death but that initial information suggested that it was as a result of a cardiac arrest.
“It is with a heavy heart that we inform the passing of Mark Groeneveld, while on a project in Hong Kong. On Monday, October 23rd, XSU and the world lost another great soul. Our deepest condolences go out to his family, team members, and friends,” the X-Speed United team wrote on its Facebook page. “We understand that this is an incredibly challenging period, and we encourage you to reach out if you need any assistance or emotional support. Your well-being is of utmost importance to us.
“While the circumstances of Mark’s passing are currently under investigation, we have received preliminary information that suggests it may have been due to a heart attack. We are working closely with the relevant authorities to gather all the facts and provide the necessary support to Mark’s family during this painful period.
“Mark was an incredible individual and a cherished member of our team. He had a remarkable spirit, always ready to lend a hand behind the scenes with his infectious smile and warm-hearted nature. His presence brightened our days, and he will be deeply missed by all who had the privilege to know him. Take care of yourselves and each other during this trying time.”
Several riders have put an end to their careers this season as a result of heart issues. Nathan Van Hooydonck, Sep Vanmarcke, Wesley Kreder, and Niklas Eg all quit during this season.
From monkey DNA (SV-40), to turbo cancer to it never being tested for quality control or outcomes. The Government, Pharma, WEF and whoever else was behind it screwed over a lot of people. Read and weep.
It’s information like this that Google and Facebook are suppressing.
EXCLUSIVE: Health Canada Confirms Undisclosed Presence of DNA Sequence in Pfizer Shot "Health Canada has confirmed the presence of a Simian Virus 40 (SV40) DNA sequence in the Pfizer COVID-19 vaccine, which the manufacturer had not previously disclosed. There is debate among… pic.twitter.com/AM3f2LOndU
“It took my breath away.” —Dr. Drew on the new study shows 50% of young men who got myocarditis after the vaccine now have permanent heart damage and he doesn’t understand why this isn’t front page news. And he recommends injured students sue any school that mandated it. pic.twitter.com/rlUgKhCS2l
In my first 67 years on this planet, I never saw a teenager, young adult, or professional athlete have a stroke or heart attack – until the mRNA Covid vaccines hit in 2021.
My first day of kindergarten at Peace Memorial School was in 1959, so you can appreciate that I have some… https://t.co/LA09CByI11
— DonaldBest.CA * DO NOT COMPLY (@DonaldBestCA) October 21, 2023
Not everyone has had the opportunity to speak with their executives. I did while working in the tech industry and have known since before 2010 that they are evil and are both spying and censoring everything they touch.
It means if you use their search engine, you get their results, not correct results.
There are plenty of alternative search engines out there. If you are reading this, I recommend you switch to one. Your results will at least be less biased and you will be less tracked.
Here is more evidence with a link to go find out for yourself. Don’t let the headline about the election fool you. They did it on Covid, DEI, and just about every other morally significant topic where they could influence your thinking.
Earlier this month, Google announced that it is partnering with fellow globalists at the World Health Organization and the United Nations to seize control of the online flow of information and push their hand-selected viewpoints to the very top of the Google search engine while suppressing independent voices.
Among other things, Google’s algorithm will work to “delete websites” that question or criticize the COVID-19 narrative, international banking, FBI crime statistics, and globalism.
Google’s censorship campaign will also look to protect massive global corporations from criticism and scrutiny. Reportedly, included in Google’s list of forbidden topics is the massive amount of waste produced by pro-trans beer brewer Anheuser-Busch.
As has become the trend in recent years, Google is presenting its massive censorship effort as a form of “fact-checking.” Google appears to have released a long list of media “partners” from all over the world who will be promoted in the search results, as they espouse Google, WHO, and UN-approved talking points.
Google’s push to squash independent media outlets plugs right into other efforts by the Big Tech corporation and its partners to stifle the free flow of information online and corral the world’s population, specifically Americans and other Westerners, into a globalist echo chamber.
As National File previously reported, the World Economic Forum and the United Nations have entered into a partnership with Google and other Big Tech firms to crush independent research and advance the climate change hoax, plus the agenda for complete and total control that goes along with it.
Melissa Fleming, the United Nation’s Under-Secretary-General for Global Communications and an advisor to the World Economic Forum, claimed in an interview that globalist organizations “own the science” on so-called climate change and have “partnered with Google” to crush independent research and dissenting viewpoints.
“For example, if you Google ‘climate change,’ you will, at the top of your search, you will get all kinds of UN resources,” said Fleming last fall.
“We’re becoming much more proactive,” said Fleming. “You know, we own the science and we think that the world should know it.”
It’s hard to imagine anyone believing the Government, Big Pharma or that the Covid Vaccine works. It’s been one lie after another including the ones about Ivermectin and Hydroxychloroquine don’t work on Covid. Another one is that the jab somehow prevents Covid, which it doesn’t.
It’s a coronavirus (cold) that 99.7% of the people survive, unlike the jab that kills far more people.
Yet here it is. SMH. These are the sheep that line up for the slaughter.
More than 7 million Americans had rolled up their sleeves for the updated COVID-19 vaccines as of Wednesday, according to the U.S. Department of Health and Human Services, despite reports that some people are still finding it difficult to book vaccination appointments or find the shots at no cost.
The updated vaccines from Moderna or Pfizer and BioNTech are single-target shots aimed at the XBB.1.5 omicron subvariant of the coronavirus, which was the dominant variant in the U.S. for much of this year but has since been overtaken as the virus continues to evolve.
Millions of doses of another updated COVID vaccine from Novavax have also been made available to Americans this week, according to the company.
Distribution of the Pfizer and Moderna shots began after the U.S. Centers for the Disease Control and Prevention recommended them on Sept. 12.
Last year’s booster targeting the original virus and another variant was rolled out about 10 days earlier. By Sept. 28, 2022, almost 7.6 million Americans had received the updated shots.
U.S. public health officials have been optimistic that Americans will get the new vaccines and have recommended that everyone ages 6 months and older receive one.
But demand has dropped sharply since 2021, when the shots were first introduced at the height of the pandemic.
About 17% of the U.S. population, or 56.5 million people, ultimately received last year’s version of the vaccines.
If they still believe the Covid vaccine actually works on the population least likely to get sick from it, you shouldn’t waste money sending kids there. They proved they don’t believe the facts or science.
No College Mandates, an advocacy group that argues against the Covid-19 vaccine for higher education, counts 79 colleges and universities that require their students to be vaccinated this fall semester.
“There are 79 colleges in the US still mandating COVID vaccines when there should be zero just like the rest of the world. Do Not Comply!” No College Mandates posted on X.
The advocacy group said “COVID injections for one of the lowest risk populations” is “insanity.” They added higher education has “zero efficacy and safety data for the the newly approved COVID injections. It is incomprehensible that this remains a reality.”
Many of these schools mandating Covid vaccines are situated in or around Democratic-controlled metro areas (map courtesy of X user Broken Truth).
If you are curious about which colleges have lifted mandates, the group has published a spreadsheet listing those institutions (read: here).
In stuff that we knew in 2020, the truth comes out about how to VERY INEXPENSIVELY AND EFFECTIVELY CURE COVID-19. After lying that it didn’t work, I guess the payoff from the vaccine companies is finished, so everyone can now admit it. Two plus billion later in payoffs, we get this:
The Mayo Clinic which has been touted by many as the best hospital system and medical research center in
the United States, recently made an interesting update on their website regarding the drug Hydroxychloroquine.
In the new update on their site, it now says “Hydroxychloroquine may be used to treat coronavirus (COVID-19) in certain hospitalized patients.”
Previously the Mayo Clinic claimed Hydroxychloroquine and chloroquine were “malaria drugs authorized for emergency use by the FDA during the COVID-19 pandemic. However, the FDA withdrew that authorization when data analysis showed that the drugs are not effective for treating COVID-19.”
Here’s Mayo Clinic’s previous stance on the drug: (Lying)
President Trump was one of the most notable figures to take Hydroxychloroquine after he tested positive for Covid-19. (because it worked, but the MSM couldn’t let him be right)
— The REAL Politically Savvy 🇺🇸 (@patriot_savvy) July 13, 2023
They couldn’t let Trump be right or they wouldn’t have been able to cheat on the election and miss a chance to snipe at him with lies.
No wonder we don’t trust Government, Medicine or Pharma anymore. And no one will ever be held accountable for the deaths that could have been prevented.
Any other time, this would be Murder by not curing patients, but that will never see the light of day.
Novak Djokovic was willing to sacrifice being the all time majors winning record holder for his health. I’ll pull for him at the US Open and other tournaments for sticking to his principles and not getting jabbed.
Aaron Rodgers wouldn’t get jabbed either, and proved it wouldn’t stop him by only missing one game when he got Covid.
Joe Rogan pissed off Big Pharma, Big Government and the other Covid commies by taking Ivermectin, HCQ, mono-clonal antibodies and beating it in 3 days.
Look at this Instagram post by Rodgers, pranking Moderna and praising another warrior.
Not a single person who didn’t get jabbed regrets it.
I guess they decided to use what worked last time. You’d think they’d be more creative. Before you read any further, I ask if you’ve learned your lesson or are going to be a sheep again.
The first source, a high-level TSA official confirmed and known to Infowars, reached out to Infowars and cited a Tuesday meeting in which TSA managers were told new memorandums & policies were being completed that would re-implement masking, starting with TSA & airport employees as early as mid-September.
The TSA official also said next week they will receive new guidelines on how the policy will escalate: by mid-October, mask-wearing will be required by pilots, flight staff, passengers, and airport patrons.
After hearing from the TSA manager, Infowars reached out to our trusted Border Patrol source who is also a manager. This source confirmed the same directives were being given to Border Patrol.
Covid-19 wastewater levels and hospitalizations have been rising from low levels for weeks, and federal data show a rise in positive tests for respiratory syncytial virus, too. Health officials expect the flu to join the mix in coming months.
For the first time, vaccines are available for all three of these illnesses, including new RSV shots for older adults and reformulated vaccines for Covid-19 and the flu.
“It’s new territory for all of us, particularly for older persons and people at high risk,” said Dr. William Schaffner, an infectious-disease physician at Vanderbilt University Medical Center.
After the dismal success of Test Run For Tyranny v1.0
in 2020-2022, an encore was never a matter of if but of when. So will “Americans” lay docilely down en masse again and take their buggering like good little sheep as they so disgracefully did last time around? Or can we expect more resistance of these blatantly contra-Constitutional edicts than we too-recently witnessed?
This “updated vaccine” is nothing to do with Eris, of course, as much as the language in the headlines implies it’s been “adapted” for the latest variant, it hasn’t.
It was in the works before Eris was even said to exist.
Moderna had the brass neck to claim that they did a “trial” showing their updated vaccine protects against Eris. Considering Eris first hit the headlines just a few weeks ago it looks like Moderna may have broken their own record in terms of speedy “trials”.
It’s just the same old slop it always was.
Hell, let’s be honest, it could be water. It could be ANYTHING.
The content of the syringe was never the important part.
After all, what you were being injected with wasn’t the point, the point was that you got injected because they told you to.
It was about forcing obedience, setting the vaccine mandate precedent and seeing how effectively people could be gaslit into taking a shot that they’d already been told they don’t need and doesn’t work.
Well, that and governments handing over VAST amounts of cash to pharmaceutical companies, obviously.
But they already have the money, and most people (allegedly) took the vaccine…so why are they still going?
You have to appreciate the huge amount of effort that went into hypnotizing millions – maybe billions – of people into acting against their own best interests, it’s a spell that’s easier to maintain than restart.
If they start letting people forget, then soon they’ll have to begin the ritual all over again.
And the magic is already wearing off.
IT’S ABOUT MAIL IN BALLOTS TO RIG THE ELECTION.
If you can’t have people come to the polls to vote (because they are too afraid), then it’s easier to have the necessary amount of mail in ballots show up at 4 AM in the morning to fix the vote count.
It’s approved now as all the payouts are done for the mRNA jabs. Is anyone going to trust the government anymore? How about the doctors that knew it worked and lied?
Oh, and Hydroxychoroquine also worked to cure Covid-19. They lied about that one also.
We knew the people pushing the vaxx knew it wasn’t safe and effective. We didn’t know that it wasn’t safe or effective, we just knew the people pushing it didn’t know either. And that was enough for me not to take it as well as a lot of others.
Doctors are free to prescribe ivermectin to treat COVID-19, a lawyer representing the U.S. Food and Drug Administration (FDA) said this week.
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, said during oral arguments on Aug. 8 in the U.S. Court of Appeals for the 5th Circuit.
The government is defending the FDA’s repeated exhortations to people to not take ivermectin for COVID-19, including a post that said “Stop it.”
The case was brought by three doctors who allege the FDA unlawfully interfered with their practice of medicine with the statements.
“The fundamental issue in this case is straightforward. After the FDA approves the human drug for sale, does it then have the authority to interfere with how that drug is used within the doctor-patient relationship? The answer is no,” Jared Kelson, representing the doctors, told the appeals court.
The FDA on Aug. 21, 2021, wrote on X, formerly known as Twitter:
“You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
The post, which linked to an FDA page that says people shouldn’t use ivermectin to prevent or treat COVID-19, went viral.
In other statements, the FDA said that ivermectin “isn’t authorized or approved to treat COVID-19” and “Q: Should I take ivermectin to prevent or treat COVID-19? A: No.”
Command or Not
“FDA made these statements in response to multiple reports of consumers being hospitalized, after self medicating with ivermectin intended for horses, which is available for purchase over the counter without the need for prescription,” Ms. Honold said.
A version of the drug for animals is available, but ivermectin is approved by the FDA for human use against diseases caused by parasites.
Ms. Honold said that the FDA didn’t purport to require anyone to do anything or to prohibit anyone from doing anything.
“What about when it said, ‘No, stop it’?” Circuit Judge Jennifer Walker Elrod, on the panel that is hearing the appeal, asked.
“Why isn’t that a command? If you were in English class, they would say that was a command.”
Ms. Honold described the statements as “merely quips.”
“Can you answer the question, please? Is that a command, ‘Stop it’?” Judge Elrod asked.
“In some contexts, those words could be construed as a command,” Ms. Honold said.
“But in this context, where FDA was simply using these words in the context of a quippy tweet meant to share its informational article, those statements do not rise to the level of a command.”
The statements “don’t prohibit doctors from prescribing ivermectin to treat COVID or for any other purpose” Ms. Honold said. She noted that the FDA, along with the statements, said that people should consult their health care providers about COVID-19 treatments and that they could take medicine if it was prescribed by the provider.
“FDA is clearly acknowledging that doctors have the authority to prescribe human ivermectin to treat COVID. So they are not interfering with the authority of doctors to prescribe drugs or to practice medicine,” she said.
Judge Elrod is on the panel with Circuit Judges Edith Brown Clement and Don Willett. All three were appointed under President Donald Trump.
Federal Law
The plaintiffs are Drs. Paul Marik, Mary Bowden, and Robert Apter. They say they were professionally harmed by the FDA’s statements, including being terminated over efforts to prescribe ivermectin to patients.
Dr. Marik has noted that a number of studies support using ivermectin against COVID-19, as the FDA itself has acknowledged. Some other studies show little to no effect.
Federal law enables the FDA to provide information, such as reports of adverse reactions to drugs, but not medical advice, Mr. Kelson said.
“This is something the FDA has never been able to do. And it’s a bright line,” he told the court, adding later:
“The clearest examples of where they have gone over the line are when they say things like, ‘You are not a horse, you are not a cow. Seriously, y’all. Stop it.’”
Judges indicated they agree that the FDA lacks the power to give medical advice; Judge Clement said, “You’re not authorized to give medical advice.”
But Ms. Honold said the government “isn’t conceding that in this case.”
She also argued that Congress has empowered the FDA to protect public health and make sure regulated products are safe and effective, giving it the “inherent authority to further its mission by communicating information to the public about safe uses of drugs.”
A ruling in favor of the doctors would prevent the FDA from reporting on consumers suffering after cooking chicken with NyQuil or that opioid addiction is a problem, she claimed.
Mr. Kelson said that wasn’t accurate. “It’s when they step beyond that [and] start telling people how they should or should not be using approved drugs,” he said.
Ms. Honold also said that the courts can’t hold agencies accountable when they provide false or misleading information: “The FDA is politically accountable, just like all other executive agencies.”
And they are debating if Covid was man made in the Wuhan labs. Hell, they were making in California.
I’m not a mice lover. I actually don’t care much other than I don’t like to see animals treated cruelly (like Fauci did with dogs). Still, it shows a tremendous lack of respect for live, both human and animals. It also shows the Chinese have a lack of respect for any retribution for doing this to us. Should we look at why the current administration allowed this? We’ve known about Covid for a while. Maybe it’s the same as a spy balloon to Washington.
Through the warrant issued by the Fresno County Department of Public Health, authorities were able to inspect a believed-to-be vacant building in Fresno County, California where they found 900 “inhumanely” treated mice. According to court documents, the Prestige BioTech representative present onsite during the investigation was identified as Wang Zhaolin, who informed the investigators that “these mice were genetically engineered to catch and carry the [Wuhan coronavirus] COVID-19 virus.”
Prestige, the company allegedly running the lab, is based out of Nevada and is the successor to Universal Meditech, Inc (UMI).
The City code enforcement stumbled upon the building at 850 I St. in Reedly in December 2022, when they discovered a garden hose running up into the building through a hole in the wall. On March 3, they obtained a warrant to inspect the property, and in April, the Fresno County public health department issued an inspection order for the illegal bio facility.
Apart from the lab rats, inspectors also found a room used to make COVID-19 tests and pregnancy tests as well as 35-plus freezers and refrigeration units that contained “thousands of bodily fluids, serums, tissues, and other medical items.”
(Photo credits: The Gateway Pundit)
The Mid Valley Times reported: “According to Assistant Director of Fresno County Public Health Humero Prado’s declaration, which was filed in superior court, investigators discovered that one room of the warehouse was used to produce COVID-19 and pregnancy tests. In other rooms, investigators found blood, tissue, and other bodily fluid samples. They also found thousands of vials that contained unlabeled fluids.” As per the court documents, a total of 48 containers – with approximately 44 gallons per container – full of biologics and medical waste were removed a day after the inspection. Another 31 were taken out the next day.
Zieba said that officials have cleared the area of hazardous materials but are still working to empty the warehouse. “Some of our federal partners still have active investigations going. I can only speak to the building side of it,” she added.
Meanwhile, David He, who is another Prestige representative, avoided inquiries on accountability and ownership of the company. He also dodged questions about whether or not they were properly disposing of the hundreds of dead mice. The firm did not even confirm if the biologics contained in the lab were theirs.
City Manager Nicole Zieba disclosed that the biotech company was operating 35 freezers and refrigeration devices without anyone questioning the electrical draw that would be required for a building that “was supposed to be vacant.” On July 5, the team entered the building and saw that the power to the freezers “was lost” but the biological samples were still frozen.
CDC discovers bacterial and viral agents in the “deserted lab”
From May 2 to 4, the Centers for Disease Control and Prevention‘s (CDC’s) Division of Select Agents and Toxins inspected the laboratory inside the “unoccupied” building. The documents confirmed that CDC found potentially infectious agents at the location, including bacterial and viral agents: chlamydia, E. Coli, streptococcus pneumonia, hepatitis B and C, herpes 1 and 5, and rubella. The agency also found samples of malaria, coronavirus, and HIV.
According to Prado, the local public health department has been “evaluating and assessing the activities of the unlicensed laboratory.” He said that all of the biological agents were destroyed by July 7 following a legal abatement process by the agency. “The evaluation required coordination and collaboration with multiple federal and state agencies to determine and classify biological and chemical contents onsite, in addition to assessing jurisdictional authority under this unique situation,” he said.
Local officials spoke with Xiuquin Yao, who was identified as the company president, through emails included in the court documents. Yao said that Prestige moved assets belonging to the defunct company UMI to the said warehouse. Officials were unable to get any California-based address for either company except for the previous Fresno location from which UMI had been evicted. “The other addresses provided for identified authorized agents were either empty offices or addresses in China that could not be verified,” court documents said.
NBC News reported that Prestige is accused of failing to comply with orders, including providing a plan for biological abatement and disposal of the materials. Emails sent to Yao and Prestige BioTech requesting comment were not immediately answered as of Thursday, July 27. Also, according to Prado, court documents indicate that the biotech company failed to provide any licensing or permit that allows experimentation or other laboratory activity.
Follow BioTerrorism.news for more news related to bioengineering and other dangerous activities “secretly” done in China-linked labs.
Were you adequately informed about the COVID-19 treatment risks and options? Were you adequately informed about the COVID-19 genetic vaccine risks? Did you have full knowledge and understanding of those risks? Did you make a decision to (or not to) voluntarily accept vaccines or medical treatment(s) for COVID-19 disease? Does your physician check in with you to insure that you are providing continuous and ongoing consent if you are participating in any experimental treatments or clinical research studies?
Were you coerced, enticed, or forced to accept an experimental medical product or procedure without providing fully informed consent?
Who is Robert Malone is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
John Allison, J.D. previously wrote and published an essay (August 2022) on the topic of COVID-19 vaccines and informed consent, and he has now updated his prior essay with additional information (updated late July 2023). Following is his updated essay, with associated references.
COVID-19 Vaccines and Informed Consent
By John Allison, J.D.
Updated July 25, 2023
Introduction.
Most Americans have long assumed that they have a fundamental right to make decisions about their own bodily health and the medical treatments they receive. Informed consent is the ethical and legal principle by which that fundamental right is enforceable. To be able to give informed consent a person needs to be informed about the risks and benefits of, and alternatives to, the proposed treatment.
The fundamental right to informed consent is particularly important with respect to the COVID-19 vaccines which are available in the United States pursuant to Emergency Use Authorizations (EUAs). Under the federal EUA statute, people are entitled to be informed about their right to accept or refuse administration of these vaccines, the consequences (if any) of refusing vaccination, and the benefits and risks of alternatives to the vaccines. A different federal statute gives the manufacturers of EUA vaccines, and the people and organizations administering them, immunity from liability suits for damages. Unless courts decide that the immunity statute cannot be applied against people who did not give their informed consent to vaccination, people who suffer severe adverse effects after receiving a COVID-19 vaccine will not be able to recover compensation, for their monetary and emotional distress damages, from the vaccine manufacturers or from the people who vaccinated them. Similarly, the family members of people who die after receiving a COVID-19 vaccine will not be able to recover compensation for their loss.
Opinions and Basis for Opinions.
Based on the results of my research to date, I have arrived at the following opinions with respect to the COVID-19 vaccines that are being widely used in the United States:
1. Government misinformation about the safety and effectiveness of the COVID-19 vaccines, censorship of credible scientific and medical information about the risks of death and serious adverse effects of the COVID-19 vaccines, and vaccination coercion, are depriving people of their ability to give informed consent to vaccination. Unless the limited effectiveness of the vaccines and the risks of death and serious adverse effects described in this memorandum are disclosed to people before they are vaccinated, informed consent has not been obtained.
2. Safe and effective drugs on the market for many years, such as ivermectin and hydroxychloroquine, have been proven by reputable doctors to be successful in the early treatment of COVID-19. If those affordable drugs had been allowed to be more widely used in the United States before people needed to be hospitalized, many tens of thousands of people who died from COVID-19 would probably be alive today.
3. The COVID-19 vaccines authorized for use in United States do not meet established criteria for establishing their short-term and long-term safety and efficacy. Serious safety signals – red flags – about these vaccines have been ignored, and continue to be ignored, by the FDA and the CDC. Also, during the past two years it has become clear that the COVID-19 vaccines do not prevent infection or transmission of COVID-19. Fully vaccinated people can become infected and can spread the SARS-CoV-2 virus to other vaccinated people and to unvaccinated people. All of these vaccines should be taken off the market immediately.
· SARS-CoV-2 is the coronavirus that causes COVID-19. Distinctive spike proteins on the surface of the virus enable the virus to penetrate cells and cause infection.
· According to a mortality analysis by the Johns Hopkins Coronavirus Resource Center, as of July 19, 2023 the United States had a COVID-19 case fatality ratio of 1.1%. The case fatality ratio is the number of deaths divided by the number of confirmed COVID-19 cases. This means that, in the United States, 98.9% of all the people with a confirmed case of COVID-19 survived the disease. Most COVID-19 deaths occurred in elderly people who were in poor health with multiple comorbidities. A study by researchers at Stanford University found that 99.9973% of COVID-19 patients 19 years of age and younger survive the disease.
· The spike proteins on the surface of the SARS-CoV-2 virus mutate, producing the Delta variant which became the dominant form of the virus by the middle of 2021. Continuing mutations of the spike proteins produced the Omicron variant which became the dominant form of the virus by the end of 2021. We are now dealing with sub-variants of Omicron.
· The first confirmed case of COVID-19 in the United States was reported in mid-January, 2020. The pandemic spread. COVID-19 vaccines were not available until the middle of December 2020 when the FDA granted emergency use authorization for the Pfizer-BioNTech and the Moderna vaccines. In February 2021 the FDA granted emergency use authorization for the Johnson & Johnson/Janssen vaccine. Early in 2021 these vaccines became widely available in the United States and mass vaccination programs began. By the middle of 2021 millions of Americans, including workers in many different occupations, were fully vaccinated.
· According to data on the CDC website accessed on July 18, 2022, in the United States there were 385,670 deaths attributed to COVID-19 in 2020 before the vaccines were widely available. In 2021, when the Pfizer-BioNTech, the Moderna and the Johnson & Johnson/Janssen vaccines were widely available and mass vaccination campaigns took place, there were 463,210 deaths attributed to COVID-19; there were 20.1% more COVID-19 deaths in 2021 than in 2020.
· The COVID-19 vaccines do not produce immunity to COVID-19 because they are not designed to trigger an immune response to the SARS-CoV-2 virus. Instead, the vaccines are designed to cause the body to produce spike proteins in order to stimulate an immune response to the spike proteins which are on the surface of the virus. The Pfizer-BioNTech and Moderna vaccines use synthetic mRNA genetic instructions to cause the body to produce enormous numbers of spike proteins. The mRNA technology used in those vaccines is a new and unproven technology that has never been used before in vaccines administered to people. The Johnson & Johnson/Janssen vaccine is a viral vector DNA vaccine that also causes the body to produce enormous numbers of spike proteins.
· An internal CDC email produced in response to a Freedom of Information Act request reveals that on January 30, 2021 the Director of the CDC had a conversation with the Director of the NIH about “vaccine breakthroughs” based on an article published in the Journal of the American Medical Association a few days earlier. “Vaccine breakthroughs” refers to fully vaccinated people who become infected with the SARS-CoV-2 virus and contract COVID-19.
· When FDA issued its EUAs for the Pfizer-BioNTech, Moderna and Johnson & Johnson/Janssen COVID-19 vaccines in late 2020 and early 2021, the CDC defined a “vaccine” as a “product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.” Traditional vaccines for diseases such as smallpox and polio meet that definition, which is consistent with the definition of “vaccine” found in the 1996 edition of Webster’s New Universal Unabridged Dictionary: “any preparation used as a preventive inoculation to confer immunity against a specific disease, usually employing an innocuous form of the disease agent, as killed or weakened bacteria or viruses, to stimulate antibody production.”
· In July 2021 an outbreak of SARS-CoV-2 infections in Barnstable County, Massachusetts led the CDC to reverse its position on the wearing of masks and to recommend that all people wear masks indoors when viral transmission is likely, regardless of their vaccination status. The outbreak involved 469 people with COVID-19 infections; 79 percent of those people were symptomatic. 74 percent of the symptomatic people were fully vaccinated. Five people needed to be hospitalized; four of the five were fully vaccinated. This incident made it clear that the vaccines do not prevent infection or transmission of COVID-19. Vaccinated people can become infected and can also spread the SARS-CoV-2 virus to other people.
· Effective September 1, 2021, once it had become clear that the COVID-19 vaccines do not produce immunity to COVID-19, the CDC simply changed its definition of “vaccine” to: “A preparation that is used to stimulate the body’s immune response against diseases.” Internal CDC emails produced in response to a Freedom of Information Act request, including an August 13, 2021 email from Andrew Lowndes at CDC to Alycia Downs at CDC, indicate that the change in definition was intended to justify continuing to refer to the COVID-19 injections as “vaccines.” Redefining the word “vaccine” does not turn these experimental products into true vaccines as the term “vaccine” has been understood by people for many years. These products are, in reality, more accurately described as gene therapy injections that cause the body to produce spike proteins. As Moderna acknowledged in its quarterly report filed with the Securities and Exchange Commission for the period ending June 30, 2020, “[c]urrently, mRNA is considered a gene therapy product by the FDA.”
· In a recent letter dated April 18, 2023 Dr. Peter Marks, Director of the FDA’s Center for Biologics Evaluation and Research, acknowledged the current FDA position “that FDA’s authorization and licensure standards for vaccines do not require demonstration of the prevention of infection or transmission. . . . There is no requirement that the vaccine also prevents infection with the pathogen that can cause the disease or transmission of that pathogen to others.”
· Project Salus, a Department of Defense and Joint Artificial Intelligence Center study, analyzed the effectiveness of mRNA COVID-19 vaccines against the Delta variant among Medicare beneficiaries 65 years and older. The project’s September 28, 2021 report indicates, on page 7, that “In this 80% vaccinated >=65 population, an estimated 71% of COVID-19 cases occurred in fully vaccinated individuals” (emphasis in the report). The report also points out, on page 12, that “In this 80% vaccinated 65+ population, an estimated 60% of COVID-19 hospitalizations occurred in fully vaccinated individuals in the week ending August 7th” (emphasis in the report).
· When the Delta and later the Omicron variants became the dominant form of the SARS-CoV-2 virus, a number of studies in different countries show that most COVID-19 hospitalizations and deaths occur among fully vaccinated people. For example, the UK Health Security Agency’s March 3, 2022 COVID-19 Vaccine Surveillance Report contains information in Table 12, on page 43, about deaths between January 31 and February 27, 2022 among patients who died within 28 days of testing positive for COVID-19 or who had COVID-19 mentioned on their death certificate. Of the 3,957 patients who died, 3,429, or 86.6%, had received two or three doses of a COVID-19 vaccine. (725 people had received two doses, and 2,704 people had received three doses.)
· Since the Omicron variant became the dominant form of SARS-CoV-2, the effectiveness of the mRNA vaccines (Pfizer and Moderna) diminishes significantly over just a few months. According to a Danish study, which has not yet been peer reviewed, vaccinated people, more than 90 days after vaccination, are significantly more likely than unvaccinated people to be infected by Omicron. A different study published in April of this year, which has been peer reviewed, found that the “risk of COVID-19 also varies by the number of vaccine doses previously received. The higher the number of vaccines previously received, the higher the risk of contracting COVID-19.”
· On July 13, 2022 the FDA granted emergency use authorization for the Novavax adjuvanted COVID-19 vaccine for people ages 18 and older, which was later amended to authorize administration of the Novavax vaccine to people ages 12 and older.
· On August 31, 2022 the FDA granted emergency use authorizations for the Pfizer-BioNTech and the Moderna bivalent (Original and Omicron BA.4 and BA.5 strains) vaccines as boosters. No clinical (human) studies were performed on those bivalent vaccines before they were authorized for emergency use. Only non-clinical studies on a relatively small number of mice were performed. On April 18, 2023 the FDA amended and expanded the emergency use authorizations for the bivalent vaccines to make them generally available, and ended the emergency use authorizations for the original (monovalent) Pfizer-BioNTech and Moderna vaccines.
· On June 1, 2023 the FDA revoked the emergency use authorization for the Johnson & Johnson/Janssen vaccine. As a result, only the Pfizer-BioNTech and Moderna bivalent vaccines, and the Novavax adjuvanted vaccine, are now available in the United States.
· The results of a study published in a peer-reviewed article on April 19, 2023 show that the bivalent vaccines have very limited effectiveness. The authors conclude that “the current bivalent vaccines were about 29% effective when the Omicron BA.4/5 lineages were the predominant circulating strains, and effectiveness was lower when the circulating strains were no longer represented in the vaccine. A protective effect could not be demonstrated when the XBB lineages were dominant.”
· Pfizer’s Comirnaty COVID-19 vaccine received full FDA approval on August 23, 2021 and Moderna’s Spikevax COVID-19 vaccine received full FDA approval on January 31, 2022. However, those vaccines have not been available in the United States. If they were available in the United States, emergency use authorizations for the COVID-19 vaccines that are available could not lawfully be maintained. Under the EUA statute, one of the mandatory criteria for an emergency use authorization is that “there is no adequate, approved, and available alternative” to the product in question. The Pfizer-BioNTech and Moderna vaccines available in the United States are legally distinct EUA products that were not transformed into approved products by the FDA’s approval of Comirnaty and Spikevax.
· It turns out that the spike proteins produced by the body in response to the COVID-19 vaccines are, themselves, toxic to cells. For example, endothelial cells line the inside of arteries to make blood flow smoothly. Damage to the endothelial cells caused by spike proteins increases the potential for microscopic blood clots to form. Those microscopic blood clots can travel to the lungs, increasing the risk of developing pulmonary arterial hypertension which is a serious progressive condition that overtaxes and weakens the heart. There is no known cure for that condition. All of the mRNA COVID-19 vaccines, as well as the Johnson & Johnson/Janssen vaccine, have been shown to cause other serious blood clotting disorders as well.
· In the mRNA COVID-19 vaccines manufactured by Pfizer and Moderna the genetic instructions that cause the body to produce spike proteins are encapsulated in lipid nanoparticles. A preclinical study on laboratory animals conducted by Pfizer and submitted to the regulatory agency in Japan shows that the lipid nanoparticles and mRNA genetic instructions enter the bloodstream and accumulate in several organs, including the spleen, bone marrow, liver and adrenal glands, and concentrate in the ovaries. The body then starts producing spike proteins wherever the mRNA genetic instructions happen to land.
· A number of serious medical conditions have been associated with the COVID-19 vaccines, including blood clotting disorders, cardiac emergencies, myocarditis, Guillain-Barré Syndrome, autoimmune disease, spontaneous miscarriages, nervous system disorders and female infertility.
· The COVID-19 vaccines also interfere with the natural immune system, making a person more susceptible to viral infections and cancer. In a May 6, 2021 preprint article, which has not yet been peer reviewed, a group of research scientists in the Netherlands and Germany reported their conclusion that the Pfizer-BioNTech vaccine “induces functional reprogramming of innate immune responses, which should be considered in the development and use of this new class of vaccines.” They also point out that “inhibition of innate immune responses may diminish anti-viral responses.” A more recent peer reviewed article published June 2022 in Food and Chemical Toxicology explains how the mRNA COVID-19 vaccines subvert innate immunity and dysregulate the body’s system “for both preventing and detecting genetically driven malignant transformation within cells.”
· A laboratory study in Sweden shows that the Pfizer-BioNtech COVID-19 vaccine is able to enter a human liver cell line where it is reverse transcribed into DNA within a matter of hours. As a result, the possibility that the COVID-19 vaccines affect DNA cannot be ruled out.
· The mRNA COVID-19 vaccines contain problematic ingredients that should not be injected into peoples’ bodies. Both the Pfizer and the Moderna vaccines contain polyethylene glycol (PEG) as an active ingredient. Several years ago, in 1993, an Expert Panel assessing the safety of PEG recommended against using PEG in ointments applied to damaged skin because some burn patients treated with a PEG-based antimicrobial cream experienced renal tubular necrosis and died of kidney failure. The PEG used in the Moderna vaccine matches the description of a PEG product manufactured by Sinopeg, a company in China. According to the Sinopeg website, that product is for “research use only.” The Moderna vaccine also contains a lipid known by the trade name SM-102. The Pfizer vaccine also contains a lipid known by the trade name ALC-0315. According to the safety information on the website of Cayman Chemical Company, which manufactures SM-102 and ALC-0315, both of those products are “for research use – Not for human or veterinary diagnostic or therapeutic use.” Yet, in the mRNA COVID-19 vaccines, PEG, and SM-102 or ALC-0315, are being directly injected into people’s bodies.
· As Dr. Peter McCullough pointed out in his October 13, 2021 sworn expert witness Declaration filed in the U. S. District Court for the Middle District of Florida: “The COVID-19 genetic vaccines (Pfizer, Moderna, J&J) skipped testing for genotoxicity, mutagenicity, teratogenicity, and oncogenicity. In other words, it is unknown whether or not these products will change human genetic material, cause birth defects, reduce fertility, or cause cancer.”
· Pfizer reportedly cut corners in the pre-clinical animal testing of the Pfizer-BioNTech COVID-19 vaccine. According to a May 28, 2021 article on the TrialSite News website, which reports on clinical trials, Pfizer performed its pre-clinical animal tests using “surrogate” mRNA instead of the mRNA that is actually in the vaccine.
· Deficiencies in the clinical trials for the Pfizer-BioNTech COVID-19 vaccine are explained in a public document prepared by the Canadian Covid Care Alliance, a group of more than 500 independent Canadian doctors, other health care practitioners and scientists. The document also contains information from six months of follow up in the Pfizer-BioNtech clinical trial, indicating that related adverse events were 300% higher in the vaccinated group than in the placebo (control) group, and severe adverse events were 75% higher in the vaccinated group than in the control group. The document can be found at:
· No long-term clinical studies were performed to evaluate the long-term safety of the COVID-19 vaccines. As a result, there is no way of knowing whether or not vaccinated people will suffer severe adverse side effects in the future. This lack of information is of particular concern since the vaccines increase the potential for developing cardiovascular disease and autoimmune disease, which can both take months or years to fully develop. Because clinical trial participants in the placebo (control) group were subsequently given the option of getting vaccinated, and a number of them chose to be vaccinated, there is no longer a statistically viable control group for a study of the long-term adverse effects of the vaccines.
· Pfizer recognizes that the long-term adverse effects of its COVID-19 vaccines are not currently known. In its Agreement to supply Pfizer-BioNTech COVID-19 vaccines to the government of a European country, Pfizer’s subsidiary required the purchasing government, in paragraph 5.5 of the Agreement, to acknowledge “that the long-term effects and the efficacy of the Vaccine are not currently known and that there may be adverse effects of the Vaccine that are not currently known.”
· The Pfizer-BioNTech, Moderna and Johnson & Johnson/Janssen COVID-19 vaccines fail to meet reasonable expectations for product uniformity. Analyses by independent researchers show that some vaccine batches, identified by lot number, are many times more toxic than others. Roughly 80% of the vaccine batches account for 1 or 2 adverse events per batch reported in the government’s Vaccine Adverse Events Reporting System (VAERS). Other batches account for hundreds or thousands of adverse events per batch reported in VAERS, and some of those adverse events involved death, disability or serious illness. A recent study in Denmark of Pfizer-BioNTech COVID-19 vaccines confirms a correlation between adverse effects and vaccine batch. For vaccines administered in Denmark between December 27, 2020 and January 11, 2022, batches comprising 4.22% of the vaccine doses accounted for 27.49% of serious adverse events, batches comprising 63.69% of the vaccine doses accounted for 71.5% of serious adverse events, and batches comprising 32.09% of the vaccine doses accounted for 1.01% of serious adverse events.
· The government established VAERS in 1990 which is co-managed by the CDC and the FDA. It is intended to be a national early warning system to detect possible safety problems with vaccines in the United States. The number of serious adverse events and deaths that have been reported in VAERS for the COVID-19 vaccines is many times greater than the serious adverse events and deaths reported in VAERS for all other vaccines combined. As of October 7, 2022 more than 31,400 deaths, and more than 230,200 serious injuries, following administration of one of the COVID-19 vaccines have been reported in VAERS. Several thousands of those deaths occurred within a day or two after vaccination. Due to underreporting, the actual number of deaths and serious injuries following COVID-19 vaccination is likely to be higher than the number reported in VAERS. Yet the CDC and the FDA continue to ignore these serious safety signals.
Click on the link to see what is happening to the jabbed. I’m sorry if you got one. All of my friends did too. The Covid jab didn’t stop Covid nor it’s transmission. It was a lie that the current administration told.
Don’t ever trust the government, the CDC, WHO, UN or any organization that says you have to do something again. It is life or death, and they choose your death.
And who comprises the deep state? The unelected. To save our country, these groups need to be eliminated. I hope for our country that somehow we can overcome the cheating, ballot harvesting and Zuckerbucks all designed to keep the very people who could easily lead us out of the mess we are in.
Everyone knows they are cheating. Everyone knows they are corrupt, but they have the backing of big money and decades of corruption all in the name of power and control. Yes, it is evil and yes, it is human nature that has played out since the beginning of man.
If not, this is how countries fall. Look at France right now. They are leaderless and are burning right now because they refused to protect their borders.







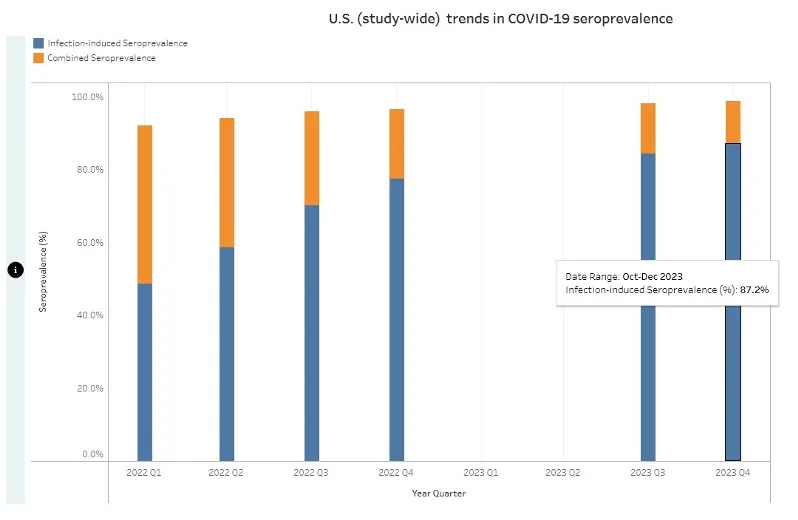






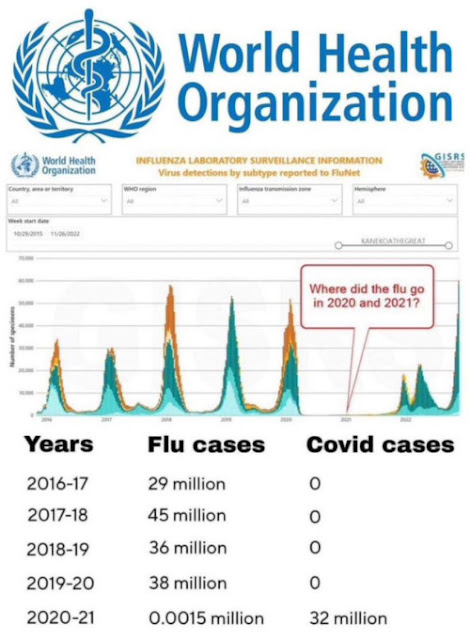











































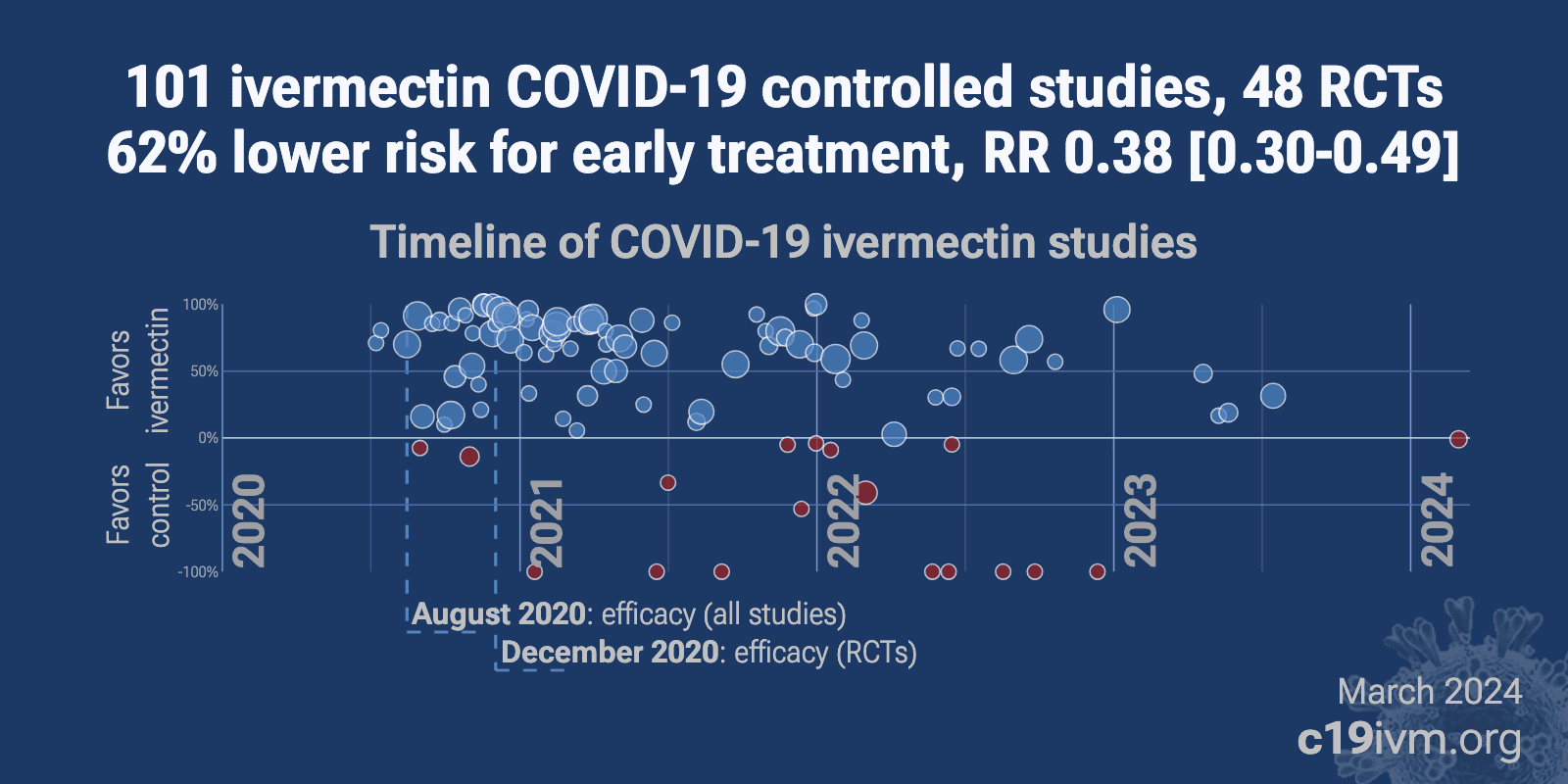
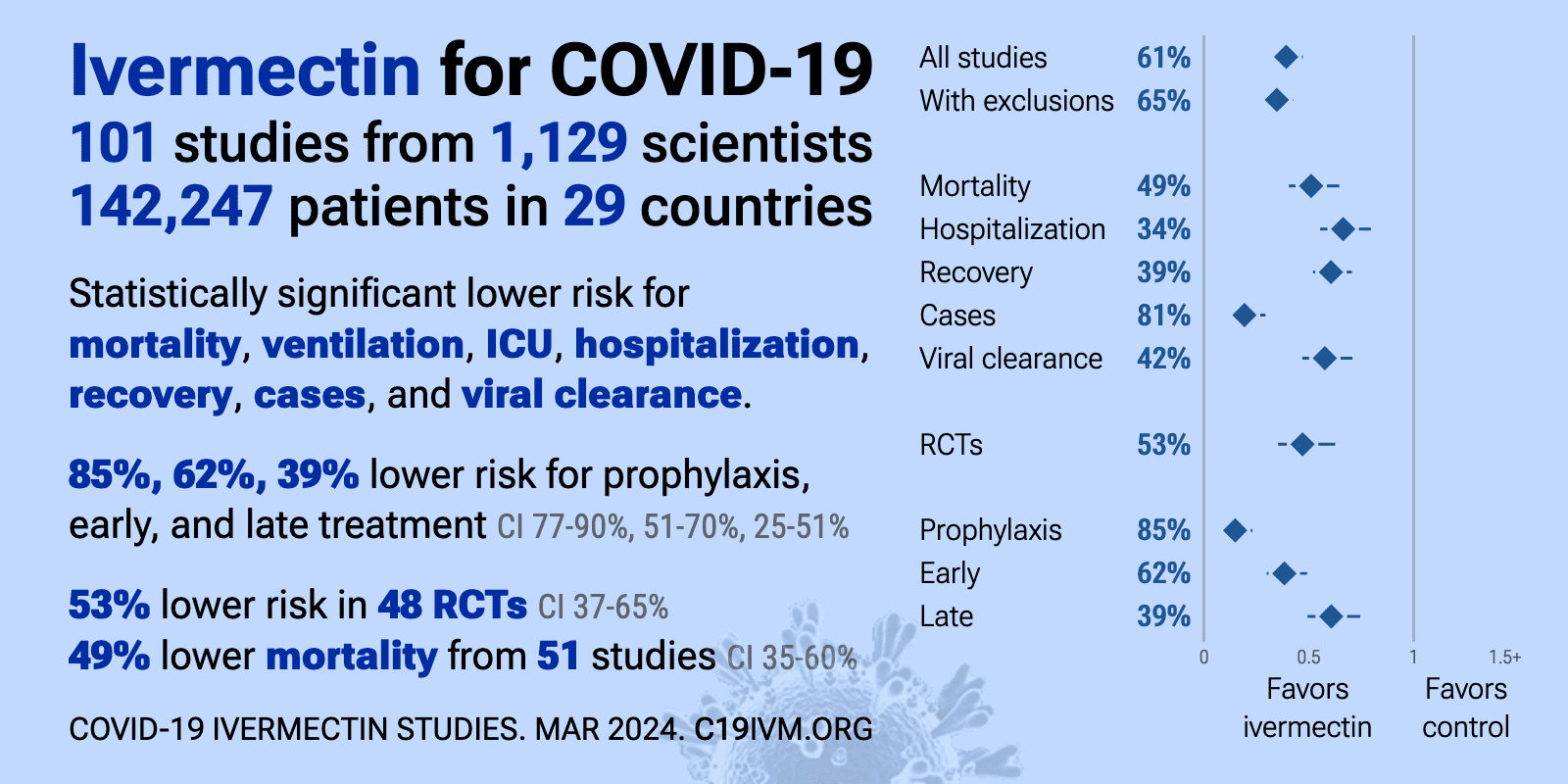














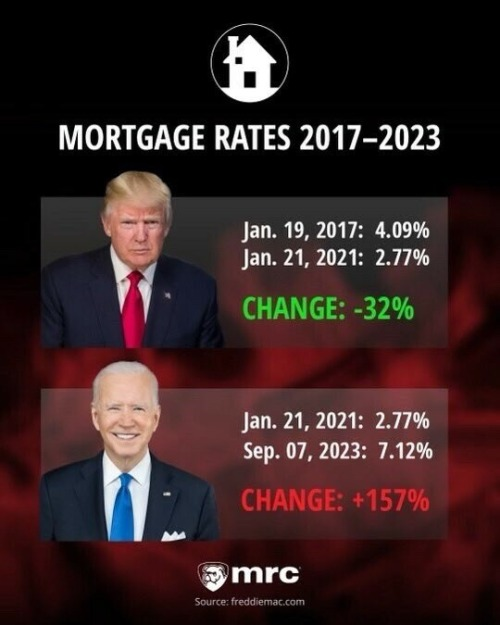



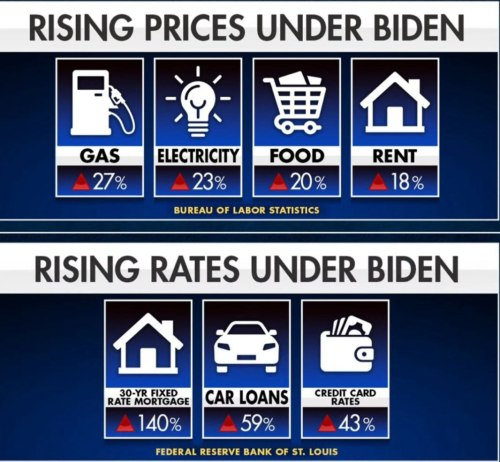


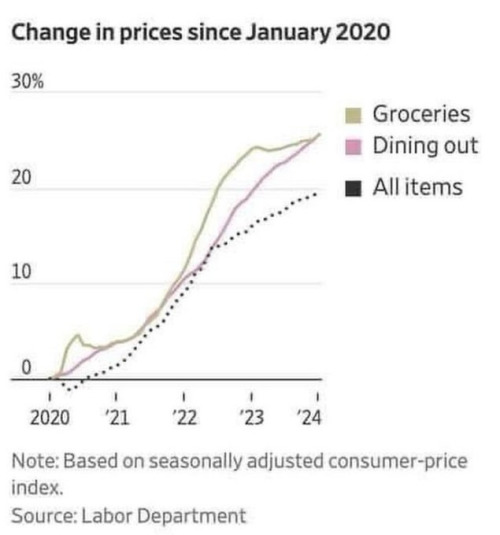



























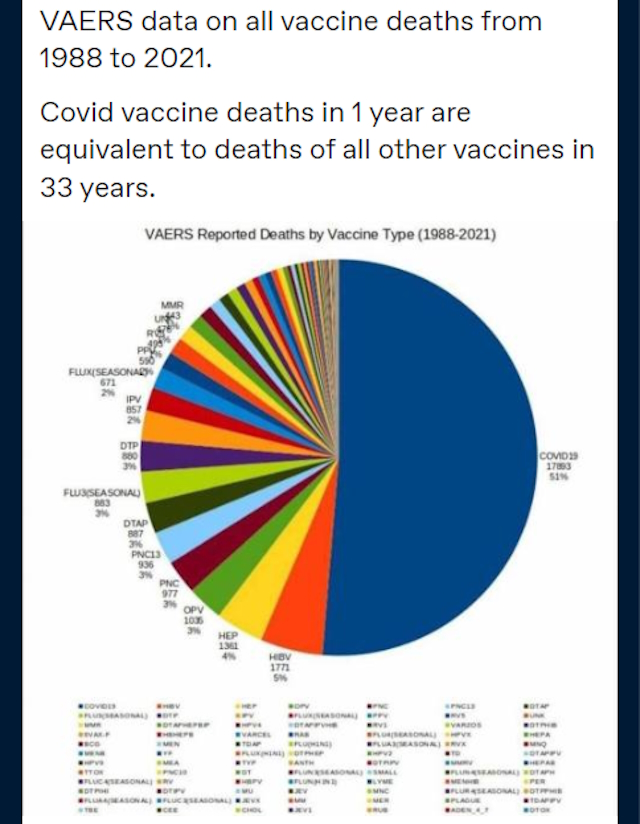

















































































.JPG)









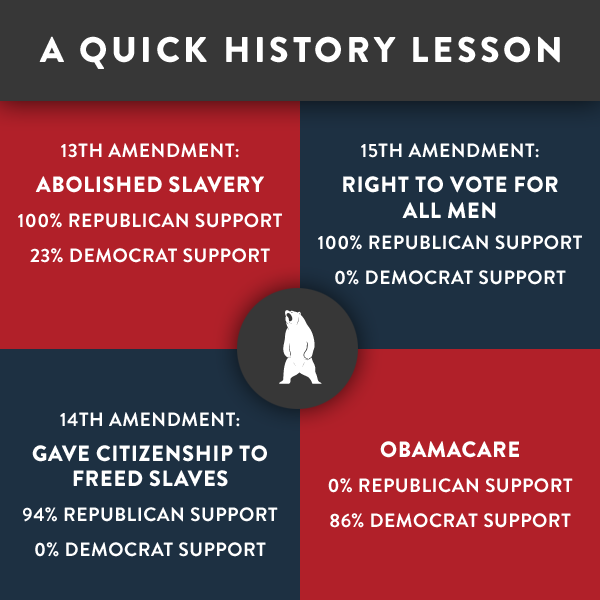























































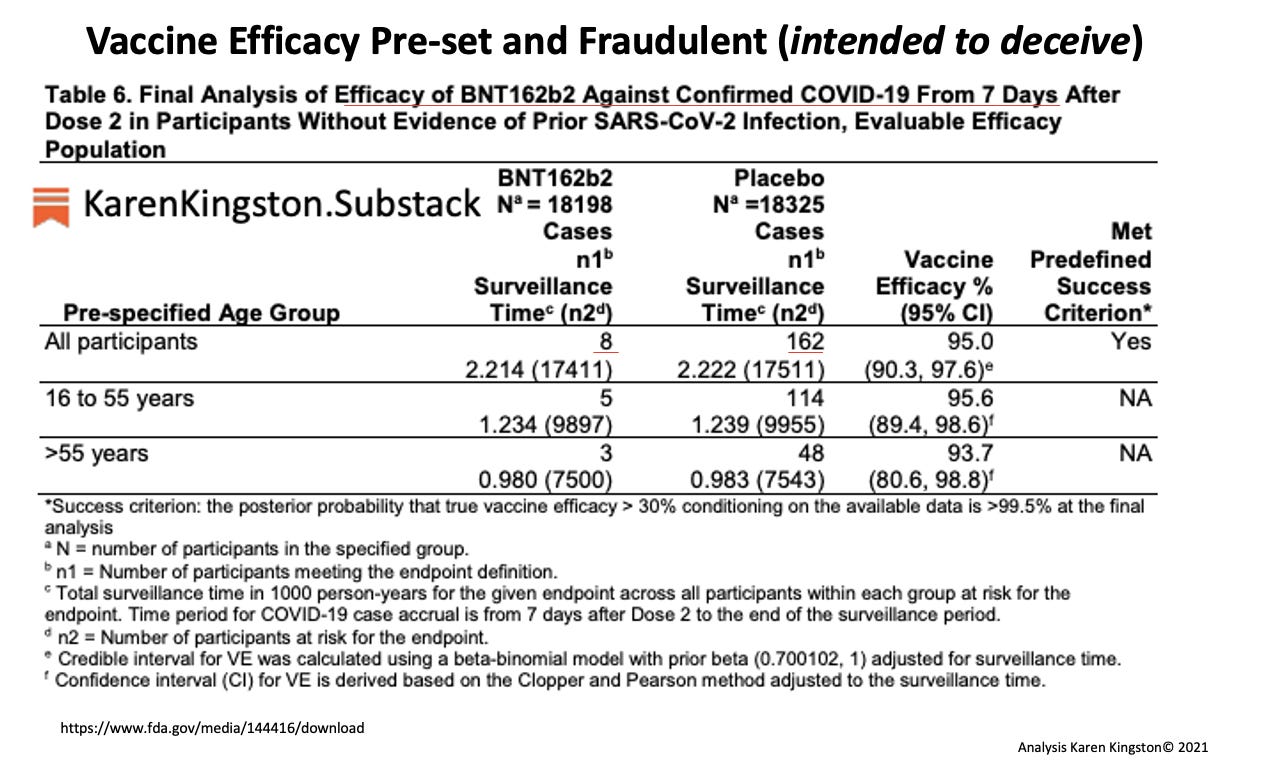
































 By
By 






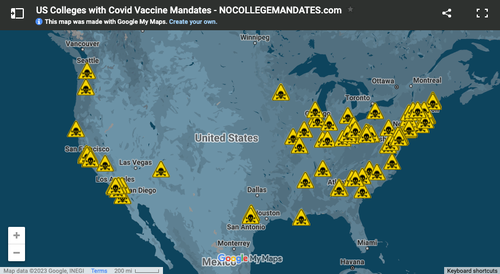

 The
The 













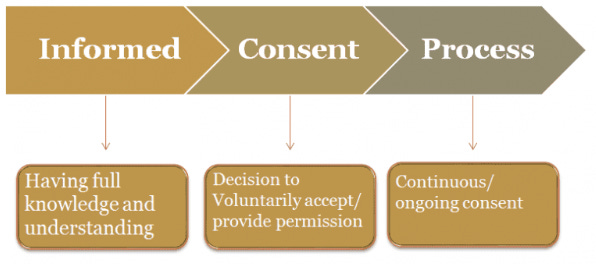









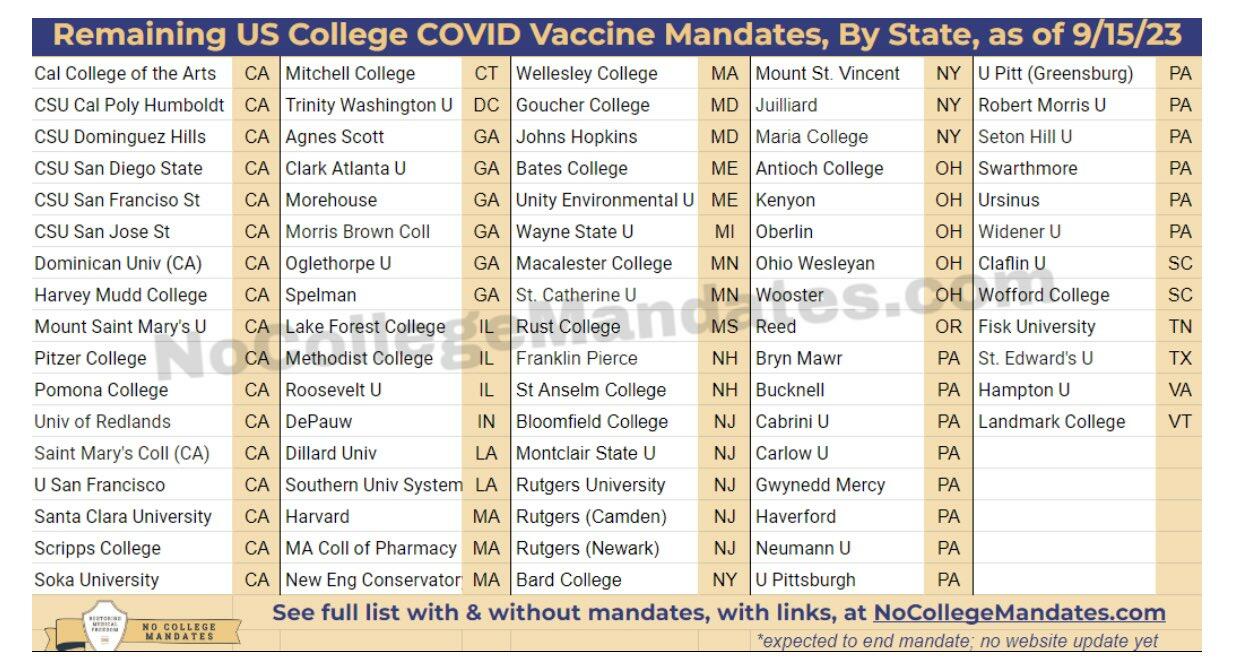{kind=link}
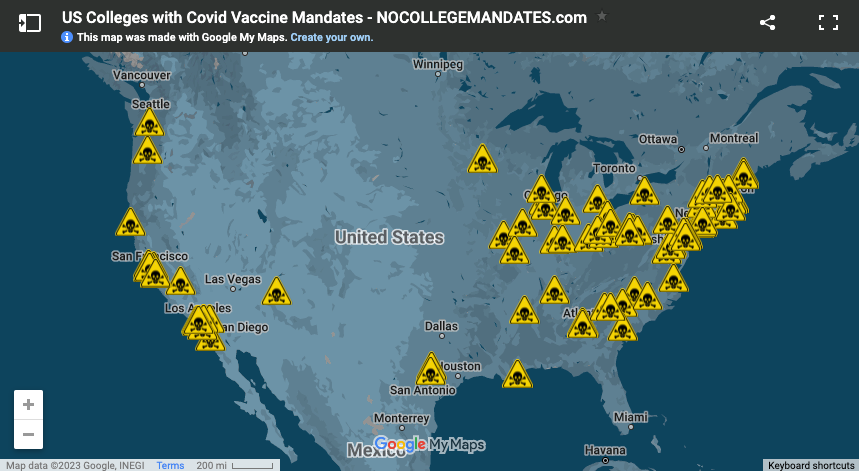{kind=link}
{kind=link}